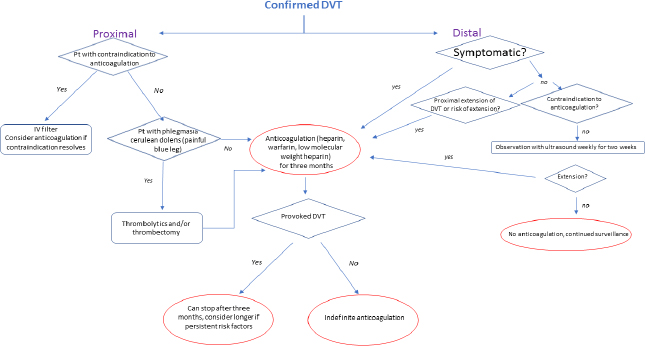
3 Venous Thromboembolism Prophylaxis Abstract This chapter will provide current best practices of venous thromboembolism (VTE) prophylaxis. VTE is a disease process that includes deep venous thrombosis (DVT) and pulmonary embolism (PE). The reader will be able to integrate recommendations from multiple sources and justify given prophylaxis protocols. Keywords: venous thromboembolism, deep venous thrombosis, pulmonary embolus, Caprini score Six Key Points • Risk stratification is based on the Caprini score. • Venous thromboembolism prophylaxis should continue for 1 month after surgery. • Risks factors include surgery, cancer, immobility, prior history, age, and obesity. • A patient with a postoperative deep venous thrombosis (DVT) should remain anticoagulated for 6 months. • A patient with a postoperative DVT should get a hypercoagulable workup. • Workup should be 6 months after event. 1. How do you risk stratify patients for venous thromboembolism (VTE)? Different methods are used for risk stratification for VTE. A common method, and one used in the plastic surgery literature reviewing VTE risk after surgery, is the Caprini score.1,2 2. Your patient had a prior VTE. How should the patient be risk stratified? According to the American College of Chest Physicians (ACCP) guidelines, the suggested risk stratification for VTE is high risk with a VTE less than 3 months prior or with severe thrombophilia, such as antiphospholipid antibodies; moderate risk includes patients who have had a VTE within 3 to 12 months and nonsevere thrombophilia, such as a heterozygous factor V mutation, recurrent VTE, or active cancer; and low risk is a prior VTE greater than 2 months ago and no other risk factors. 3. What are known risk factors for VTE? Known risk factors for VTE are surgery, cancer, immobilization, prior history, age, and obesity.3 Virchow’s triad includes venous stasis, vascular injury, and/or hypercoagulability. Surgery itself causes venous stasis, because of vasodilation from general anesthesia and after intravenous saline infusion.4 Vascular injury can occur during surgery, and other risk factors are documented in the Caprini score. 4. How long should patients be on postoperative VTE prophylaxis? For patients undergoing major abdominal surgery, a Cochrane review5 indicated that prophylaxis should be given for 1 month after surgery. The review was based on three randomized controlled trials in manuscript form, and one randomized controlled trial in abstract form. They noted that a benefit of fewer symptomatic VTE was found in prolonged prophylactic therapy, without an increase in the risk of bleeding. Postoperative enoxaparin has been shown to be beneficial in high-risk plastic surgery patients.6 5. Your patient is postoperative day (POD) 6 after body contouring for massive weight loss and call the office with reports of right calf tenderness. He reports he was working out the day prior and thinks he may have strained his calf muscle, and would like to take a muscle relaxant with his pain medication. What do you do? This patient should go to the emergency room to rule out a DVT, which can present as calf tenderness. Workup should include a Doppler ultrasound. A high-sensitivity D dimer is often used in the workup of DVT, but can be elevated after recent surgery. 6. What sequelae can patients get after DVT? The most feared event after a DVT is a pulmonary embolus (PE), which has a fatality risk. Even without PE, patients can get phlegmasia alba dolens (white swollen leg), phlegmasia cerulean dolens (blue swollen leg), venous gangrene, and postthrombotic syndrome, which is characterized by pain and leg swelling.7 7. How long should patients be on anticoagulation therapy after a DVT? Patients should be on anticoagulation for at least 3 months after a DVT, and up to 6 to 12 months depending on risk factors (Fig. 3.1). 8. Should patients have a workup for a hypercoagulable state after a DVT? Patients with a DVT after surgery should have a workup, especially if it was unexpected. Because the presence of a thrombus and the use of anticoagulation can interfere with the workup, it is best to perform the workup 6 months after the event, after treatment has been completed.
Questions
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine