Vascular anomalies come in all shapes and sizes. They may be flat or raised and purple, red, or pink. They have been the subject of superstition and folklore for eons. Early attempts at classification of vascular lesions were hampered by the use of confusing, often eponymous nomenclature, based variably on clinical, pathologic, biological, embryological, or descriptive factors. An early pathologic classification by Virchow1 divided vascular anomalies into angiomas (simplex, cavernosum, and racemosum) and lymphangiomas (simplex, cavernosum, and cystoids). Conversely, a capillary malformation (CM) was variably described as a “port-wine stain,” “nevus flammus,” or “capillary hemangioma.”
Mulliken and Glowacki2 further defined the nature of vascular anomalies in a seminal work and classified these into hemangiomas and vascular malformations, distinguishing them based on clinical course, biologic behavior, and histopathological features. This laid the groundwork for our current understanding of these lesions. In 1993, Jackson et al.3 further divided vascular anomalies into hemangiomas, vascular malformations, and lymphatic malformations (LMs).
Most recently in 1996, the International Society for the Study of Vascular Anomalies (ISSVA) proposed a classification (Table 21.1) based on that originally published by Mulliken and Glowacki, which divides vascular anomalies into vascular tumors and malformations.4 This is now the most widely accepted classification system and forms the basis for diagnosing and treating vascular anomalies. Vascular tumors include hemangiomas and other proliferative lesions. Vascular malformations are subdivided based on vascular components into simple and combined malformations. Integral variants of vascular malformations include capillary, venous, arteriovenous, and lymphatic malformations. Tumors and malformations are distinguished based on biological behavior, clinical appearance, and radiological and pathological features.
Vascular tumors proliferate largely by endothelial cell hyperplasia. The prototypical lesion is the infantile hemangioma(IH), which demonstrates rapid postnatal growth andslow regression during childhood. Vascular malformations, in contrast, have a quiescent endothelium and are thought to be caused by local defects of vascular morphogenesis and remodeling. Vascular malformations never regress and often persistor enlarge throughout life. Vascular malformations have been further categorized based on flow characteristics into fast-flow and slow-flow lesions. Fast-flow lesions include lesions with an arterial component (AM [arterial malformation], AVM [arteriovenous malformation], AVF [arteriovenous fistula], C-AVM [capillary arteriovenous malformation], and L-AVM [lymphatic arteriovenous malformation]). Slow-flow lesions would encompass all other lesions.
INFANTILE HEMANGIOMA
Overview
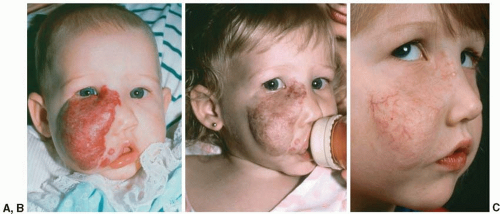
IH is a vascular tumor that affects from 5% to 10% of Caucasian infants by 1 year of age. It is more common in females than in males (3 to 5:1) and in preterm infants (23%). Around 80% of hemangiomas are solitary, while 20% are multifocal. IH is characterized by a three-stage life cycle, consisting of the proliferating phase, involuting phase, and involuted phase (Figure 21.1).
TABLE 21.1 INTERNATIONAL SOCIETY FOR THE STUDY OF VASCULAR ANOMALIES CLASSIFICATION OF VASCULAR ANOMALIES
The cellular origin of IH has been shown to be related to clonal expansion of a hemangioma-initiating multipotent stem cell,5 which expresses the marker CD133 and has the capacity to form human blood vessels expressing erythrocyte-type glucose transporter protein-1 (GLUT-1) and merosin. This vasculogenic activity appears to be confined to hemangioma-derived stem cells only. Hemangioma endothelial cells also appear to be fundamentally different from normal endothelial cells, with constitutive low expression of vascular endothelial growth factor receptor (VEGFR)1 and missense mutations in genes encoding VEGFR2 and TEM8 (tumor endothelial marker 8), suggesting a germline mutation leading to variant downstream signaling in the vascular endothelial growth factor (VEGF) pathway.6 The unique cellular nature of hemangioma cells suggests that the etiology of IH relates to a mutation of endothelial cells at the stem cell level instead of embolized placental cells, as previously postulated.
FIGURE 21.1. Hemangioma. This girl with a right facial hemangioma demonstrates the three-stage life cycle of IH, consisting of the proliferating phase ((A) age 3 months), involuting phase ((B) age 18 months), and involuted phase ((C) age 7 years).
A characteristic marker of IH is GLUT-1. IH immunostains positively for GLUT-1 throughout its life cycle and is negative in most other vascular lesions. In the proliferative phase, IH consists of plump, rapidly dividing endothelial cells, and pericytes that form tightly packed sinusoidal channels. A characteristic ultrastructural feature of this phase is the presence of multilaminated basement membranes. Increased angiogenesis is seen in this phase as documented by the expression of VEGF, matrix metalloproteinase (MMP)-2, proliferating cell nuclear antigen, and basic fibroblast growth factor. These markers of angiogenesis and cell proliferation are not seen in vascular malformations.
In the involuting phase, there is gradually decreasing endothelial activity and luminal enlargement. Apoptosis is seen in endothelial cells before 1 year and peaks in 2-year-old specimens. Increasing fibrosis, stromal cells (such as mast cells, fibroblasts, and macrophages), and expression of tissue inhibitor of metalloproteinase-1, a suppressor of new blood vessel formation, is seen.7 Finally, in the involuted phase, the previously highly cellular lesion has been largely replaced by loose fibrofatty tissue mixed with dense collagen and reticular fibers.
Clinical Features
Hemangiomas typically appear at birth or within the first 2 weeks of life. Most of these are innocuous, with only about 10% being locally invasive, disfiguring, or life-threatening. The clinical appearance depends on depth, location, and stage of evolution. Around 30% to 40% are quiescent at birth, appearing only as a cutaneous mark, such as a pale area, macular stain, telangiectatic macule, or ecchymotic spot or scratch.
The current morphological classification system for hemangiomas separates them as localized, segmental, or multiple. Localized hemangiomas present as focal, tumor-like growths that are contained to one defined cutaneous region and fail to demonstrate a linear or geometric pattern. Segmental hemangiomas are less common than the localized lesions and are generally more plaquelike in presentation. Segmental lesions also demonstrate a geographic distribution over a specific cutaneous region and are more likely to be associated with various complications, require more aggressive therapy, and have a poorer overall outcome.
Proliferative Phase.
In typical hemangiomas, the majority of proliferation occurs during a rapid growth phase in thefirst 6 to 8 months with cessation of growth by 1 year ofage. At this stage, the tumor is typically in its most florid presentation. The composition of the tumor becomes more apparent as it proliferates, demonstrating a superficial and/or deep component. The clinical presentation of the superficial component includes a bright red, well-demarcated, slightly elevated noncompressible plaque. Hemangiomas deeper in the dermis and subcutaneous tissue are usually soft, warm, ill-defined subcutaneous masses that have a slightly bluish hue. Often, hemangiomas have both superficial and deep components.
Involuting Phase.
In the involuting phase, the florid crimson color of IH fades to a dull purplish hue, with increased pallor of the skin and decreased turgor of the tumor. This phase marks the regression of the tumor, and typically lasts anywhere from 2 to 10 years. In many children the involuting phase results in virtually normal skin, but in a number of cases children with hemangiomas will exhibit residual telangiectasias, pallor, atrophy, textural changes, and sometimes residual fibrofatty tissue.
Involuted Phase.
Regression is complete in 50% of childrenby 5 years and in 70% of children by 7 years, with continuedimprovement up to 10 to 12 years of age. Bulky and large lesions may regress completely, while a flat superficial hemangioma may lead to permanent alteration in the texture of the skin.
Complications
While most hemangiomas resolve without complication, a considerable number result in functional impairment or permanent disfigurement. Ulceration is the most frequent complication,8 occurring in 5% of all cutaneous hemangiomas, and results in pain with the risk of infection, hemorrhage, and scarring. Those at greatest risk are large, segmental lesions of the lip, perineum, or intertriginous regions. Ulceration results from necrosis and usually occurs during a period of rapid growth. In addition to rapidly enlarging hemangiomas, ulceration has a high risk of occurrence in the anogenital region due to moisture and frictional stress, which results in extreme pain on urination and defecation.
Location also plays a major role in determining the likelihood of complications. Hemangiomas of the eyelid or in the periocular region can cause astigmatism, strabismus, and, in severe cases, amblyopia. Large hemangiomas on the pinna of the ear can cause deformation of the external ear or temporary conductive hearing loss. Hemangiomas with a distribution over the mandible, chin, and upper neck (“beard” distribution) have a greater risk of association with airway hemangiomas. Hemangiomas of the airway may be life-threatening because of their potential for proliferation and eventual airway obstruction. Infants with subglottic hemangiomas often present with hoarseness and stridor. These lesions in infants 6 to 12 weeks old are of particular concern as they may progress rapidly to respiratory failure.
In rare cases, multiple (usually greater than five) cutaneous hemangiomas (diffuse hemangiomatosis) and large facial hemangiomas are associated with visceral hemangiomas. These infants present from birth to 16 weeks of age with a triad consisting of congestive heart failure, hepatomegaly, and anemia, resulting in higher morbidity and mortality rates. An association between hepatic hemangiomas and hypothyroidism has also been reported, due to the production of type 3 iodothyronine deiodinase by the tumor. Hence, thyroid-stimulating hormone levels should be monitored in these infants. While the liver is the most common internal organ involved, the gastrointestinal tract, brain, and lung are also common sites.
Congenital Hemangiomas
These lesions are a unique subset of vascular tumors, distinct from IHs. Unlike IH, these rare lesions present fully grown at birth and do not demonstrate the rapid neonatal proliferation characteristic of IH. These can be classified into rapidlyinvoluting congenital hemangioma (RICH) and noninvolutingcongenital hemangioma (NICH).
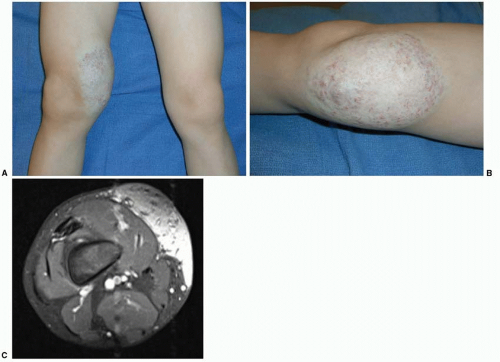
These lesions do not stain for GLUT-1, but have similar location, size, appearance, gender ratio, and histological and radiological features as IH.9 RICH manifests as a solitary raised gray or violaceous tumor with ectasia, radial veins, central telangiectasias, and a pale surrounding halo. It can result in sufficient shunting to cause high-output congestive cardiac failure. RICH’s defining feature is accelerated regression, usually obvious within a few weeks after birth and complete by 6 to 14 months of age. NICH presents as a well-circumscribed, plaquelike tumor with a pink, blue, or purple hue, central coarse telangiectasia, and a pale rim (21.2). In contrast to RICH, NICH grows proportionately to the child and remains unchanged, demonstrating a fast-flow signal by Doppler examination. There are rare instances of coexistence of either RICH or NICH in a child with IH and also instances in which RICH ceases to regress and assumes the likeness of NICH.
FIGURE 21.2. Non-involuting congenital hemangioma. A. A 1 year-old boy with noninvoluting congenital hemangioma (NICH) involving the right thigh diagnosed at birth. B. Characteristic morphology is that of a well-circumscribed, plaquelike tumor with a pink, blue, or purple hue, central coarse telangiectasia, and a pale rim. C. MRI demonstrates lesion to involve the skin and subcutaneous tissues superficial to the muscle fascia.
Differential Diagnoses
While the clinical phases of proliferation and involution usually make the diagnosis clear, a deep lesion in the neck or trunk may cause confusion with an LM. Similarly, a superficial hemangioma in an extremity may resemble a CM. In these cases, ultrasonography or magnetic resonance imaging (MRI) may be useful to confirm a diagnosis. RICH and NICH can also be mistaken for AVMs due to a prominent fast-flow signal. Another differential is pyogenic granuloma, which unlike hemangiomas rarely appears before 6 months of age (mean age 6.7 years). These lesions grow rapidly and may form a stalk or pedicle with epidermal breakdown. Other infantile tumors that may cause confusion include kaposiform hemangioendothelioma, tufted angioma, (“angioblastoma of Nakagawa”), myofibromatosis (“infantile hemangiopericytoma”), and fibrosarcoma.
Radiological Characteristics
Ultrasonography of a proliferating-phase hemangioma demonstrates a distinct shunting pattern, consisting of decreased arterial resistance and increased venous velocity. Even an experienced ultrasonographer can have difficulty distinguishing a young hemangioma from an AVM because both are rheologically fast flow. An MRI with contrast is the gold standard imaging modality, but it requires sedation or general anesthesia if the child is younger than 6 years old. MRI reveals parenchymatous (solid) tissue of intermediate intensity on T1-weighted spin-echo images and moderate hyperintensity on T2-weighted spin-echo images. Prominent flow-voids are located around and within the tumor, indicating rapid flow in feeding arteries and dilated draining veins. At some time in the late involuting phase, hemangiomas become slow-flow lesions, often with prominent fatty parenchyma.
Association with Dysmorphic Features
There are instances in which hemangiomas appear to be associated with certain dysmorphic conditions. Large facial hemangiomas of the neck and face, for instance, may be associated with a syndrome referred to as PHACES: posterior fossa malformations, hemangiomas of the cervicofacial region, arterial anomalies, cardiac anomalies, eye abnormalities, and occasionally sternal defects (Table 21.2). The large facial hemangioma is usually plaquelike and segmental in nature. There is a marked female predominance (ratio of affected girls to boys, 9:1), which is significantly greater than the 3:1 ratio of girls to boys reported for typical hemangiomas. Figure 21.3 shows a patient with PHACES who presents with the characteristic facial hemangioma accompanied by significant abnormalities in the cerebrovascular circulation.
Dandy-Walker malformation is the most common structural brain abnormality associated with PHACES. However, other central nervous system lesions have been shown. Common arterial abnormalities of the head and neck include agenesis, hypoplasia, stenosis, dysplasia, aneurysms, and anomalous branches of the major cerebral arteries. Incidence is unknown but potential neurologic defects such as developmental delay or seizure disorder, Horner syndrome, stroke, and progressive neurologic disease have been reported. Cardiac abnormalities include coarctation of the transverse aorta, but congenital heart defects such as ventricular septal defects and patent ductus arteriosus may also be seen. Eye abnormalities include optic nerve hypoplasia, persistent retinal vessels, and microphthalmia. Sporadic reports of endocrinopathies, including hypothyroidism and hypopituitarism, and intracranial hemangiomas associated with PHACE can also be found in the literature.
Hemangiomas located over the lumbosacral spine appear to also be a component of abnormal morphogenesis as they may be associated with occult spinal dysraphism or genitourinary anomalies. Of greatest concern are those lumbosacral hemangiomas that appear segmental, span the midline, and are flat or telangiectatic. Early detection and therapeutic or surgical intervention are important to prevent permanent neurologic sequelae.
Management
The management of hemangiomas remains controversial, with a large and growing number of medical and surgical modalities. Due to the wide spectrum of clinical presentation and the potential for rapid change in early infancy, it can be challenging to predict which hemangiomas will be innocuous and which will be problematic. While the decision to treat hemangiomasthat impair function or are life-threatening, suchas those occurring in the periocular region, airway, liver orgastrointestinal tract, is obvious, the decision to treat less-threateninghemangiomas often depends on the location of thehemangioma, size, and growth phase as well as the age of thepatient at the time of evaluation.
Observation.
The majority of IH will involute with time, leaving normal or slightly blemished skin only. Reassurance of the parents and regular follow-up visits are essential to monitor for local complications and progression of the hemangioma.
Local Wound Care.
Management and treatment of ulcerated hemangiomas should focus on healing the open wound, preventing secondary infections, and alleviating pain. Local wound care may include compresses for gentle debridement of thick crust and exudate reduction, barrier creams, such as zinc oxide or hydrophilic petroleum, applied to the surface of the hemangioma, and occlusive dressings to serve as barriers and prevent desiccation. Viscous lidocaine may help control pain. Topical antibiotics may be efficacious for superficial ulcerations, whereas oral antibiotics may be necessary if overt secondary infection is present and oral pain medicines may be required for pain.
TABLE 21.2 ANOMALIES ASSOCIATED WITH HEMANGIOMAS
▪
CATEGORY OF ANOMALY
▪
ANOMALY
Structural brain
Posterior fossa
Dandy-Walker complex
Cerebellar hypoplasia/atrophy
Subependymal and arachnoid cysts
Hypoplasia or agenesis of
Cerebrum
Corpus callosum
Septum pellucidum
Vermis
Absent foramen lacerum
Polymicrogyria
Microcephaly
Heterotopia
Absent pituitary or partially empty sella turcica
Cerebrovascular
Dysplasia of the large cerebral arteries
Stenosis, occlusion, absence, or moderate to severe hypoplasia of the large cerebral arteries
Aberrant origin or course of the large cerebral arteries