V-Y Advancement Flaps for Nasal Reconstruction
Julian J. Pribaz
Simon G. Talbot
DEFINITION
There are multiple different types of V-Y flaps. It is important to differentiate these especially with respect to their use in nasal reconstruction, as they must be applied correctly for successful outcome:
A classic V-Y flap refers to a triangle-shaped island flap designed at one edge of a defect with the tapering V part distal to the defect (FIG 1A).
It is based on a mobile subcutaneous pedicle.
As the triangular flap is advanced into the defect, the residual donor site is closed primarily, resulting in a Y-shaped scar.
The extended V-Y flap is a modification of the V-Y advancement flap, with the addition of an extension limb onto the advancing edge of the standard flap (FIG 1B).
The limb is located adjacent to the area requiring reconstruction and is elevated from its bed and hinged down as a transposition flap on the end of the V-Y advancement flap to close the most distal part of the defect.
A double extended V-Y flap is an even larger flap, with an extension limb on each side of the defect, so that both limbs are transposed onto the advancing edge of the V-Y flap, which itself is based on a mobile subcutaneous pedicle.3
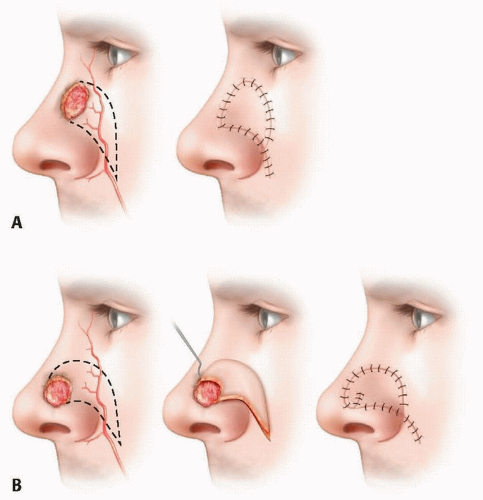
FIG 1 • Perforator V-Y flaps based on the angular artery, showing a regular V-Y design for a more vertically oriented defect (A) and an extended V-Y design for a more medial and circular defect (B).
The V-Y perforator flap is an entirely different concept, and the only similarity with the above is that the eventual donor-site closure goes from a V to a Y configuration.
Unlike the regular V-Y flaps, the perforator flaps are not based on a broad mobile subcutaneous pedicle but rather on specific perforating vessels that must be mobilized for flap advancement.
ANATOMY
The cutaneous anatomy of the nose is not uniform.
The skin in the upper half is thinner and has a variable amount of underlying subcutaneous fat, with the most mobility over the nasal bridge just below the glabella.
The lower half of the nose is thicker and more sebaceous and also much more adherent with very little mobility due to lack of subcutaneous fat.
The blood supply is rich and comes from the paired angular arteries and accompanying veins.
The angular artery starts at the alar base as a continuation of the facial artery and runs in the trough between the nasal side wall and adjacent cheek. It anastomoses with the infraorbital, infratrochlear, and dorsal nasal vessels and across the midline with corresponding vessels on the opposite side. It gives multiple small perforators that pass both medially onto the nose and laterally onto the cheek (FIG 2).4
There is relatively loose areolar tissue with some fat around the pedicle, which provides flap mobility.
The type of V-Y flap that can be used successfully will depend on the location of the defect on the nose.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients present with small, yet often challenging, defects of the nose that are usually the result of tumor excision.
In many cases, these patients have undergone Mohs surgery involving complete excision of the tumor with clear microscopic margins, making it safe to proceed with immediate reconstruction.
The location, size, shape, and orientation of the defect are important in determining the method of reconstruction.
The goal is to restore the nose to as near normal as possible, especially with respect to the contour restoration with no distortion to the natural landmarks of the nose.
Any surgery will produce scars, but contour restoration is more important because scars do settle and mature with time to becoming less conspicuous.
Ideally, the use of adjacent local tissue will ensure that the best color and texture will be restored.
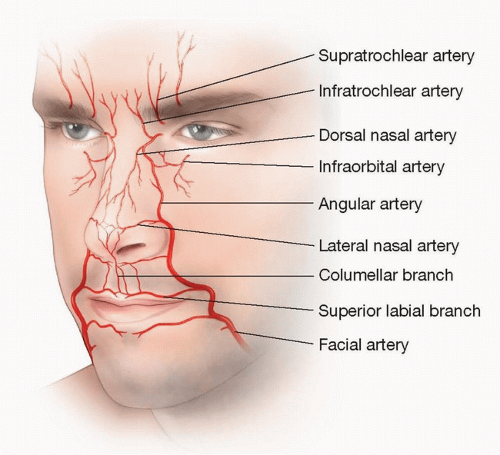
FIG 2 • Vascular supply to the nose. The angular artery starts at the alar base as a continuation of the facial artery and runs in the trough between the nasal side wall and adjacent cheek. It anastomoses with the infraorbital, infratrochlear, and dorsal nasal vessels and across the midline with corresponding vessels on the opposite side.
The use of V-Y advancement flaps brings in local “like tissue” that causes a minimum distortion.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree