Clinical Presentation
A 52-year-old White male had a “large” melanoma in the right temporal area ( Fig. 2.1 ) and underwent a wide local excision of the temporal melanoma with a 2-cm margin and sentinel lymph node biopsy in the face and neck by the surgical oncology service. He had a 4.5 × 4.5 cm skin defect down to the superficial temporal fascia involving the upper face, temporal area, and cheek ( Fig. 2.2 ). The plastic surgery service was asked to close this large skin defect after the wide local excision and sentinel lymph node biopsy.


Operative Plan and Special Considerations
Based on the size and location of the skin defect and the existing incision for sentinel lymph node biopsy in the face and neck, and skin laxity in his neck, a large cervicofacial flap was designed for this patient. The procedure itself would be similar to a classic skin-only face lift performed by plastic surgeons for facial rejuvenation. In this procedure, the excess lower face and neck skin could be dissected free and used to reconstruct the large skin defect in the upper face and temporal area. Therefore, the defect could be closed primarily and no skin graft would be needed.
Operative Procedures
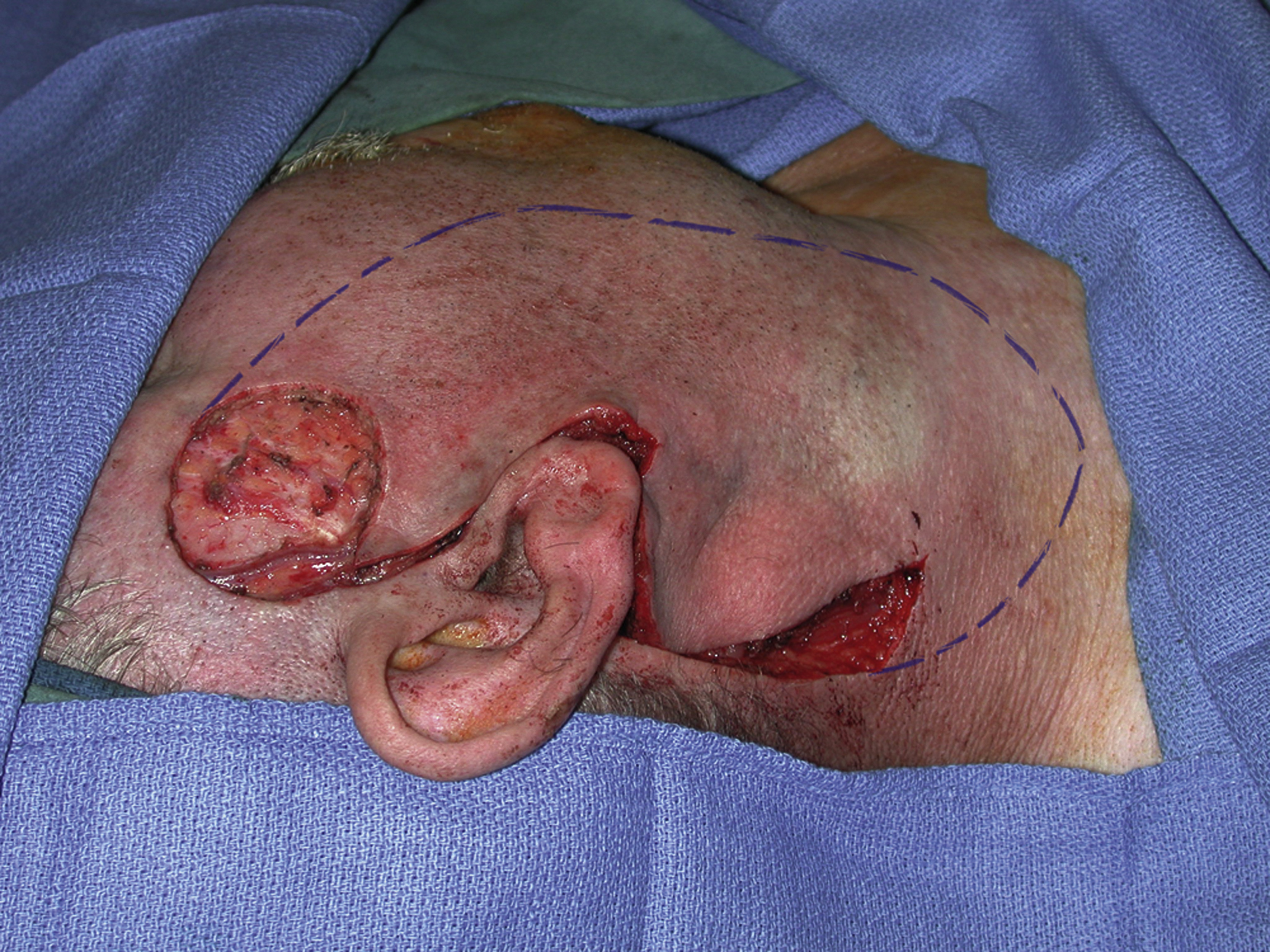
The cervicofacial skin rotation and advancement flap was designed based on the existing incision on the same side of the face and neck. The extent of the skin flap dissection was marked ( Fig. 2.3 ). Its dissection should be extensive enough for the defect to be closed without very much tension. All proposed skin dissection areas were then infiltrated with 1% lidocaine with 1:100,000 epinephrine. The skin flap dissection was performed first from inside the defect and then followed to the existing face and neck incisions. Face lift scissors can be used to facilitate skin flap elevation. The extent of the cervicofacial flap dissect for this patient was similar to a unilateral face lift surgery, superomedially toward the orbicularis oculi muscle, medially to the nasolabial fold, inferiorly several centimeters below the mandibular boarder toward the midline. If necessary, cervical skin dissection could be more extensive both medially and inferiorly. The entire cervicofacial flap was then rotated and advanced to the skin defect and excess skin of the flap was trimmed. All closure was performed in two layers including the preauricular and neck incisions as for a standard face lift incision closure. A 7-mm JP drain was inserted under the flap ( Fig. 2.4 ).