Introduction
The many specialized structures of the hand and upper extremity work in intimate synchrony to provide a harmonious interplay of precision motor biomechanics with fine tactile senses. Our hands are subject to many common occupational and domestic injuries, including fingertip trauma, tendon lacerations, neurovascular compromise, fractures, and soft tissue loss. Every extremity trauma has its own unique characteristics that offer challenges for soft tissue coverage. Although the principles of the reconstructive ladder apply, this chapter focuses on soft tissue reconstruction of the upper extremity using local, regional, and free flaps only.
Preoperative Considerations
All trauma surgeries start with patient stabilization, wound irrigation and debridement, repair and reconstruction of the skeleton and soft tissues, and culminates with definitive closure. The closure decision should incorporate the goals and priorities of reconstruction. Each area of the upper extremity has its own set of unique soft tissue needs that allow that area to function at an optimum level. Soft tissue reconstruction of the upper extremity could be divided up into six main areas ( Box 20.1 ). A final category would add catastrophic injuries such as the mangled or mutilated upper extremity where the zone of injury transcends many of the six zones in the limb.
- •
Fingertips
- •
Digits
- •
Hand
- •
Forearm
- •
Elbow/antecubital fossa
- •
Upper arm
While the goals include life preservation, limb preservation, function preservation, and then functional reconstruction, the priorities of function, contour, and stability, as well as the anticipation of further reconstructive surgery is very important in choosing the flap of choice. Currently used flaps include fasciocutaneous, fascial, musculocutaneous, muscle, and osteocutaneous flaps. Flap selection is based on the characteristics of the defect, including size, shape, and location, the availability of donor sites, and the goals of reconstruction.
Reconstruction by Region
Finger Soft Tissue Reconstruction
Finger reconstruction with flaps traditionally uses adjacent tissue on the finger, tissue from the proximal digit, the adjacent digits, the dorsal or palmar hand, or from distant tissue such as the abdomen or toe pulp. The fingertip is an area where local flaps is commonly used for reconstruction. Box 20.2 illustrates the variety of flaps available for closure of the fingertip injuries.
- •
Volar V-Y
- •
Lateral V-Y
- •
Cross finger
- •
Thenar crease
- •
Moberg volar advancement
- •
Homodigital
- •
Heterodigital
- •
Reverse dorsal metacarpal artery
- •
Thoraco-epigastric
- •
Free toe pulp/nail bed
Distal Fingertip Reconstruction
The Volar V-Y Advancement (Atasoy or Kleinart) Flap
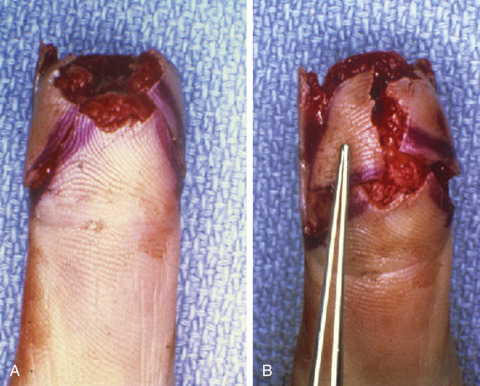
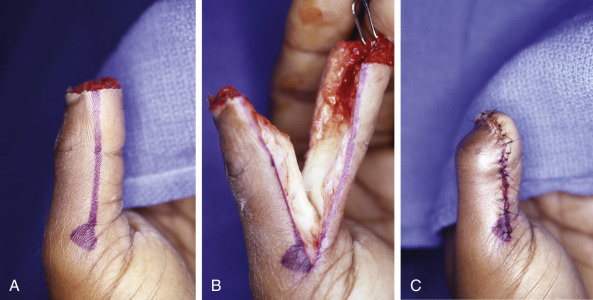
This flap is used for distal fingertip defects oriented in a dorsal oblique or transverse fashion, measuring <1 cm, usually with exposed bone. The volar triangular flap is oriented with the apex at the distal interphalangeal crease ( Fig. 20.1 ). The skin is incised full thickness. Blunt dissection with spreading of the tissue in the direction of vascular inflow into the flap is performed until the tissue advances to cover the defect. The donor site is sutured to provide a V-Y, tension free closure ( Fig. 20.2 ). Flap length is 1.5–2 times the width, and width is limited to that of the nail bed to prevent tip flattening. This flap provides durable, glabrous, sensate skin for coverage. The flap is limited to cover smaller defects usually <1.5 cm in size. Potential complications include cold intolerance, scarring, and sensory changes.


Distal Fingertip Transverse and Oblique Defect Reconstruction
Lateral V-Y Advancement (Kutler) Flaps
Transverse and dorsal oblique defects of the fingertip can occasionally be closed with a laterally based V-Y advancement with the apex at the DIP joint ( Fig. 20.3 ). It is oriented to be at least 2–3 mm from the nail folds dorsally, with a more thorough dorsal dissection to release the fibrous septae, while preserving the more volar neurovascular contributions. This again provides vascularized, sensate coverage but is severely limited in advancement to about 0.5–0.75 cm.
Distal Thumb Reconstruction
The Volar Advancement (Moberg) Flap
This flap is most often used for the thumb. Radial and ulnar midaxial incisions are made on either side of the thumb. The flap is elevated in the plane above the tendon sheath incorporating both the neurovascular bundles in the fasciocutaneous flap. The Moberg flap offers up to 2 cm of advancement to cover distal thumb defects. Occasionally the interphalangeal joint needs to be flexed to allow the flap to be inset into the remaining nailbed. The interphalangeal joint extends over time, stretching the flap as it does so. The Moberg advancement flap provides well-vascularized, glabrous, sensate coverage ( Fig. 20.4 ). There has been a number of modifications of the Moberg that are employed to provide a little more length to the advancement. The flap can be advanced as a V-Y flap where the apex is at the volar, proximal thumb crease. Alternatively, a transverse incision can be made in the skin at the proximal thumb, the tissue spread to release the tension from the more proximal palmar skin. A skin graft is then used to close to proximal donor defect as the flap advances distally. The Moberg, volar advancement flap as described is not typically used for other digits of the hand as it may cause flexion contractures of the finger.
Volar and Dorsal Digit Reconstruction
The Cross Finger Flap
The cross for your flap offers a two-stage approach to reconstruction of the volar and dorsal aspect of digits including the fingertip. The classic cross finger flap utilizes the skin and subcutaneous tissue on the dorsum of the adjacent finger at level of the middle phalanx. It is based on the dorsally migrating vessels that arise from the volar digital arteries. The venae comitantes and other superficial veins are left within the flap. Occasionally, sensory nerves can also be incorporated in the flap to provide sensation. The flap is elevated at the level of the paratenon which must be kept intact for a skin graft to be utilized over the donor site once the flap is inset. Just as in a page of a book, the flap is folded over to cover the volar defect of the adjacent finger ( Fig. 20.5 ). The flap will remain attached to the donor and the recipient fingers for 2–3 weeks, when the flap is divided and inset. The donor site is covered with a split thickness skin graft and the bolster dressing applied for the first week to provide adequate engraftment.
The reverse cross finger flap is used to cover dorsal defects on the adjacent finger. The flap is outlined on the dorsum of the donor finger but is de-epithelialized before it is transposed to the adjacent finger. A split thickness skin graft is used to cover the undersurface of the exposed flap as well as the donor site. The flap is divided and inset at 2–3 weeks.
Distal Fingertip Reconstruction
The Thenar Crease Flap
The thenar crease flap employs the skin from the volar aspect of the thumb at the level of the metacarpal phalangeal joint. The flap is based on the radial aspect of the thumb and can measure 1.5 cm in width and up to 2 cm in length ( Fig. 20.6 ). The digit with the fingertip defect is flexed down towards the elevated flap which is sutured in place. The base of the flap is divided in 2–3 weeks. The thenar crease flap is insensate and may result in flexion contractures to the recipient finger if used in adults.
Fingertip and Distal Finger Reconstruction
Homodigital and Heterodigital Flaps
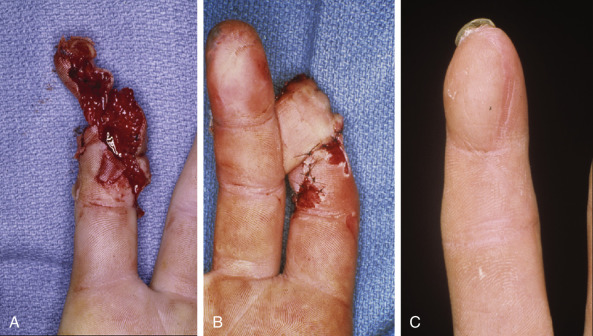
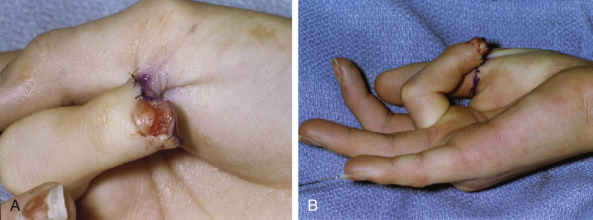
Homodigital and heterodigital flaps are usually axial flaps that are elevated in and antegrade or retrograde fashion, based on the digital artery ( Figs 20.7 , 20.8 ). Care must be taken to preserve the digital nerves so that sensation to the distal aspect of the donor finger is not compromised.


The Thoraco-Epigastric Flap
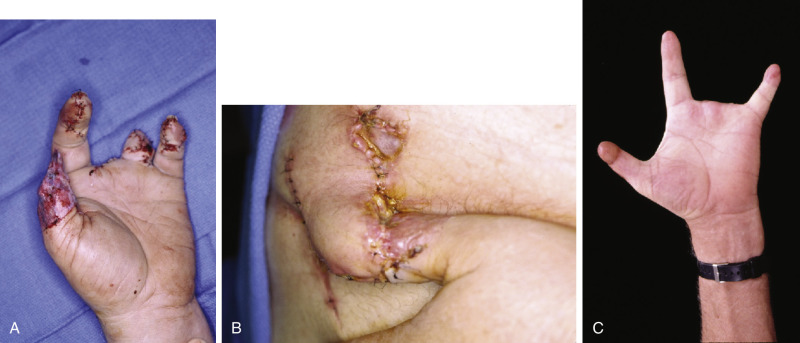
It is very uncommon in current surgical practice to apply the principles of the thoraco-epigastric flaps for closure fingertip injuries. Small flaps are raised on the trunk to allow the fingertips to be sutured to them ( Fig. 20.9 ). The patient must hold their arm in the position shown for 2–3 weeks until the flap is divided; these flaps are often bulky and remain insensate.
The Free Toe Pulp Flap
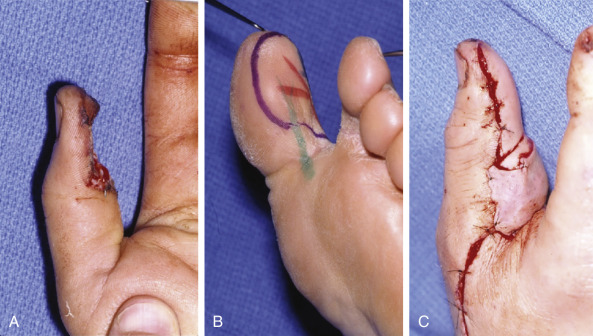
The free toe pulp flap utilizes the lateral aspect of the great toe but incorporates the glamorous skin, subcutaneous tissue, and neurovascular bundle. The flap is harvested as a free tissue transfer ( Fig. 20.10 ). Although this flap replaces the defect in the finger with like tissue, it does involve greater technical skills of fine microsurgery. Potential pitfalls include complete loss of the flop due to thrombosis in the anastomosed vessels, poor sensibility recovery, or neuroma formation. Patients may also need to be hospitalized for 5–7 days until the fate of the flap is fully known.
Volar and Dorsal Finger Reconstruction
The Dorsal Metacarpal Artery Flap
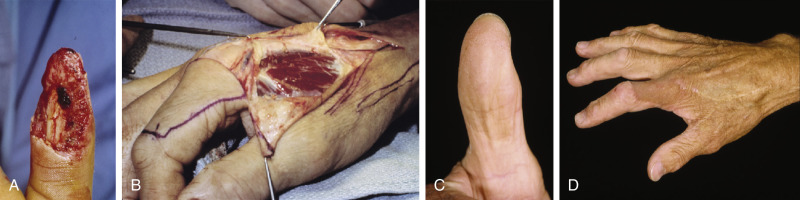
The first dorsal metacarpal artery flap is used primarily to provide durable sensate tissue to the volar aspect of the thumb. The flap incorporates the first dorsal metacarpal artery that lies within the fascia of the first dorsal interosseous muscle ( Fig. 20.11 ). The artery and superficial veins provide the inflow and venous drainage of the fasciocutaneous portion of the flap which is taken from the dorsal aspect of the proximal phalanx on the index finger. The pedicle is dissected proximally to a point where the flap can be transposed either through a tunnel or through open access to the volar thumb. The arc of rotation of the flap makes it extremely versatile to cover not only the volar thumb but also dorsal aspect of the thumb and hand. Sensation is provided by branches of the superficial radial nerve.
The reverse dorsal metacarpal artery flap can also be utilized to cover defects on the dorsal or volar aspect of the digits and even fingertip. The flap is based at the level of the metacarpal phalangeal joint in the web space, where perforating vessels from the Palmer vasculature communicate with the dorsal metacarpal artery system. The flap is therefore a distally based flap ( Fig. 20.12 ). The superficial veins must be incorporated in the flap to provide adequate venous outflow. The skin paddle is taken from the proximal aspect of the dorsum of the hand in between the metacarpals. A 1 cm wide strip is fashioned that includes the dorsal metacarpal artery must be taken to prevent vascular compromise to the flap. A Doppler must be used to identify the dorsal metacarpal artery prior to elevation of the flap. The more ulnar the dorsal metacarpal artery the less reliable its presence is within the fascia. The reverse dorsal metacarpal artery flap may be prone to venous congestion because the venous blood is forced to drain retrograde. Loose closure of the flap may help the flap until it redirects the outflow. Alternatively, a superficial dorsal vein could be anastomosed in the digit.

Dorsal and Palmar Hand Defect Reconstruction
Soft tissue coverage of the hand can be challenging. The Palmer side of the hand has glabrous skin that needs to be extremely durable and able to tolerate significant shear forces when grasping objects or holding items in the hand.
The dorsum of the hand is very thin and provides durable coverage for the gliding extensor tendons. Soft tissue defects therefore should be covered with flaps that are thin, durable and provide glide for the underlying tendons. Box 20.3 lists a variety of flaps that are locally and regionally available for coverage of defects to the hand.
Fasciocutaneous
- •
Radial forearm
- •
Ulnar artery
- •
Lateral arm
- •
Deltoid
- •
Medial arm
- •
Scapular
- •
Parascapular
- •
Thoracodorsal artery perforator
- •
Deep inferior epigastric perforator
- •
Superior gluteal artery perforator
- •
Inferior gluteal artery perforator
- •
Anterolateral thigh
- •
Anteromedial thigh
- •
Medial plantar artery instep
- •
Supraclavicular
- •
First dorsal metacarpal artery
Muscle Flaps
- •
Rectus abdominis
- •
Rectus femoris
- •
Vastus lateralis
- •
Gracilis
- •
Latissimus
- •
Serratus
Myocutaneous
- •
Transverse rectus abdominis myocutaneous
- •
Vertical rectus abdominis myocutaneous
- •
Anterolateral thigh
- •
Vertical gracilis
- •
Transverse upper gracilis
- •
Latissimus
Fascia
- •
Anterolateral thigh
- •
Scapular
- •
Lateral arm
- •
Radial forearm
- •
Serratus anterior
- •
Temporal parietal
- •
Dorsalis pedis
Osteocutaneous
- •
Fibula
- •
Scapula
- •
Radial forearm
- •
Second metatarsal
- •
Iliac crest
- •
Lateral arm
- •
Anterolateral thigh
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


