There are currently 5 botulinumtoxin-a products approved for cosmetic use in the United States: onabotulinumtoxin-a, abobotulinumtoxin-a, incobotulinumtoxin-a, prabotulinumtoxin-a, and daxibotulinumtoxin-a. New neuromodulators are destined for the market place soon including a serotype E and 2 additional serotype A botulinumtoxins. Optimizing esthetic use of neuromodulators relies on an intimate knowledge of anatomy. By altering one’s injection technique, the risk of brow ptosis can be minimized. Neuromodulators can contribute to lifting of the upper face and minimizing infraorbital hallows when injected strategically in the lower face. Contouring off-face musculature has become popular.
Key points
- •
There are currently 5 botulinumtoxin-a products approved for cosmetic use in the United States: onabotulinumtoxin-a, abobotulinumtoxin-a, incobotulinumtoxin-a, prabotulinumtoxin-a, and daxibotulinumtoxin-a.
- •
New neuromodulators are destined for the market place soon including a serotype E and 2 additional serotype A botulinumtoxins.
- •
Optimizing esthetic use of neuromodulators relies on an intimate knowledge of anatomy.
- •
Neuromodulators can contribute to lifting of the upper face and minimizing infraorbital hallows when injected strategically in the lower face.
- •
Treating pregnant and lactating patients with neuromodulators remains controversial but knowing how to appropriately counsel these individuals regarding whether to treat or not to treat is imperative.
Introduction
Neuromodulators are one of the most common cosmetic treatments that patients seek and that practitioners perform. Onabotulinumtoxin-a (Botox Cosmetic; Allergan Aesthetics; Irvine, CA) was first approved by the US Food and Drug Administration (FDA) in 2002[ ] for cosmetic use for the improvement of glabellar lines, and since that time there has been 2 additional indications for lateral canthal lines in 2013 and forehead lines in 2017. Additionally, there has been 4 subsequent botulinumtoxin type A neuromodulators that have been approved in the United States for glabellar lines—abobotulinumtoxin-a (Dysport; Galderma; Fort Worth, TX) approved in 2009, incobotulinumtoxin-a (Xeomin; Merz North America, Inc.; Raleigh, NC) approved in 2011, prabotulinumtoxin-a (Jeuveau; Evolus; Newport Beach, CA) approved in 2019, and daxibotulinumtoxin-a (Daxxify; Revance Aesthetics; Nashville, TN) in 2022 ( Table 1 ). This article will provide an overview on recent updates within the neuromodulator space including a review on yet to be approved neuromodulators as well as innovative clinical uses.
| Onabotulinumtoxin-a | Abobotulinumtoxin-a | Incobotulinumtoxin-a | Prabotulinumtoxin-a | Daxibotulinumtoxin-a | |
|---|---|---|---|---|---|
| FDA approval |
| Glabellar lines (2009) − 50 U | Glabellar lines (2011) − 20 U | Glabellar lines (2019) − 20 U | Glaber lines (2022) − 40 U |
| Active ingredients | Botulinumtoxin-a+ Neurotoxin-associated protein (900 kDa) | Botulinumtoxin-a+ Neurotoxin-associated protein (500–900 kDa) | Botulinumtoxin-a (150 kDa) | Botulinumtoxin-a+ Neurotoxin-associated protein (900 kDa) |
|
| Amount of active toxin in on-label dose for glabellar lines | 0.18 ng (20 U) | 0.27 ng (50 U) | 0.08 ng (20 U) | 0.12 ng (20 U) | 0.18 ng (40 U) |
| Equivalents to Botox units | 1:1 | 1 Ona ∼ 2–3 (∼2.5) Abo | 1 Ona ∼ 1 (∼1.25–1.5) Inco | 1 Ona ∼ 2 Pra | 1 Ona ∼ 2 Daxi |
New neuromodulators
Daxibotulinumtoxin-a is the newest neuromodulator to be approved by the FDA for cosmetic use. Please refer to article, which will provide a detailed perspective on this neuromodulator.
Although there are currently 5 different neuromodulators available in the United States for cosmetic use for a practitioner to choose from, many new neuromodulators will be approved in the coming years. Letibotulinumtoxin-a (Hugel, Inc.; Seoul, South Korea and CROMA Pharma; Leobendorf, Austria) is a botulinumtoxin-a derived from Clostridium botulinum strain CBFC26 [ , ]. This neuromodulator is already approved for glabellar lines in China, Thailand, India, Mongolia, the Philippines, and Indonesia [ ]. The product is supplied as a freeze-dried neurotoxin that requires refrigerated storage; nonpreserved saline is used for reconstitution [ ]. In a placebo-controlled phase III clinical trial conducted at 7 centers across the United States and Europe, subjects in the study group received 20 U of letibotulinumtoxin-a injected into the glabella [ ]. Four units (0.1 cc) of the active product was injected into each of 5 injection points, 2 injections into each corrugator supercilli muscle and 1 injection into the procerus muscle [ ]. This study demonstrated that 78.6% subjects treated with letibotulinumtoxin-a were responders, 1-point or greater improvement on glabellar line severity score, at 4 weeks compared with 0% of subjects in the control group [ ]. The study demonstrated that the drug lasts approximately 16 weeks [ ]. Additionally, there was a fast onset of action with 44.5% and 74.5% of subjects having a 1-point or greater improvement on glabellar line severity score within 24 hours and 3 days, respectively [ ]. The only adverse events reported were similar to other well-studied botulinumtoxins for cosmetic use [ ]. There were 3 cases of eyelid ptosis and 1 case of brow ptosis reported [ ]. No neutralizing antibodies were detected [ ]. In a randomized study conducted in Korea, letibotulinumtoxin-a was compared with onabotulinumtoxin-a for improvement of glabellar lines and ultimately demonstrated that letibotulinumtoxin-a was not inferior to onabotulinumtoxin-a and both had similar safety profiles consistent with earlier neuromodulator studies [ ]. Letibotulinumtoxin-a had a similar response rate to onabotulinumtoxin at maximal frown at all time points within the study [ ].
Another new botulinumtoxin type A that is unique in its formulation is relabotulinumtoxin-a (Galderma; Fort Worth, TX), which is supplied in a ready-to-use liquid that eliminates reconstitution before administration [ ]. When it comes to market, this will be the first ready-to-use neuromodulator that hopes to potentially increase accuracy by limiting variability and errors during the reconstitution process [ ]. This new neuromodulator was extensively studied in 2 phase III clinical trials investigating the use for glabellar lines (READY-1) and lateral canthal lines (READY-2) [ , ]. In the READY-1 study, 300 subjects were enrolled for 6 months to determine the safety and efficacy of a single dose of 50 U of relabotulinumtoxin-a for moderate-to-severe glabellar lines [ ]. This investigation demonstrated a rapid onset of action, with approximately 39% of subjects reporting improvement in glabellar lines within 1 day of injection [ ]. The median onset of glabellar line improvement was 2 days [ ]. Ninety-eight percent of subjects demonstrated a 1-grade or greater improvement of glabellar lines compared with baseline at maximal frown at 1 month postinjection and 58% of subjects maintained this response at 6 months [ ]. Approximately 80% of subjects treated with relabotulinumtoxin-a did not return to baseline glabellar lines within 24 weeks [ ]. The safety profile was in alignment with other neuromodulators, headache was the most common treatment-related adverse event, and there was only 2 reported cases of eyelid ptosis [ ]. A 60 U dose of relabotulinumtoxin-a was studied for improvement of moderate-to-severe lateral canthal lines in the READY-2 trial, which also enrolled approximately 300 subjects [ ]. Similarly to the READY-1 trial, the READY-2 trial demonstrated a fast onset of action with 34% of subjects reporting improvement of their lateral canthal lines as early as 1 day postinjection [ ]. The median time to onset of improvement of these lines was 2 days [ ]. Ninety-three percent of treated subjects had a 1-grade or greater improvement of lateral canthal lines from baseline at maximal smile at month 1 with 36% of subjects maintaining this response at 6 months [ ]. Approximately 60% of subjects treated with relabotulinumtoxin-a did not return to their baseline level of lateral canthal lines within 24 weeks [ ].
Another novel neuromodulator is a serotype E botulinumtoxin [ ]. Botulinumtoxin type E has the same molecular mechanism of action as serotype A; however, it has the fastest onset of action and the shortest duration of all botulinumtoxins [ ]. Similar to type A, type E consists of a 100-kDa heavy chain and a 50-kDa light chain [ ]. Both types A and E inhibit neuromuscular transmission by cleaving synaptosomal-associated protein 25 but at different cleavage points [ ]. In a randomized, double-blinded clinical trial, this type E botulinumtoxin was studied in a dose escalation manner for the improvement of moderate-to-severe glabellar lines [ ]. The neuromodulator was administered in the standard 5-point injection technique into the procerus and corrugators muscles [ ]. It was found that botulinumtoxin type E had onset of clinical effect within 24 hours and a duration of effect ranging between 14 and 30 days dependent on the dose administered [ ]. Importantly, this new drug demonstrated no serious adverse effects, the most common adverse event was mild headache [ ]. It is yet to be determined where this drug will fit into the marketplace. One hypothesis of how this product could potentially be used includes for use in patients who are treatment naïve in the cosmetic space wishing to try a neuromodulator before committing to a longer duration of effect. Another potential use for this product is therapeutically, either before or after skin surgery to help potentially limit scarring by reducing muscular tension on a suture site.
Biosimilars are starting to enter the pharmaceutical realm most powerfully in the biologics market. Neuromodulators could potentially be the next drug category that could see emerging biosimilars take hold. In a noninferiority, phase III clinical study, a biosimilar abobotulinumtoxin-a (Dyston; Imen Vaccine Alborz; Iran) was compared to abobotulinumtoxin-a (Dysport; Galderma; Fort Worth, TX) for the treatment of moderate-to-severe glabellar lines [ ]. This study demonstrated that the biosimilar was effective and not inferior to abobotulinumtoxin-a [ ]. Moreover, the treatment with the biosimilar was demonstrated to be safe [ ].
Updated face techniques
Since onabotulinumtoxin-a was approved for improvement of glabellar lines, our understanding and usage of this and other neuromodulators has become more sophisticated; and in turn, results for patients have improved. Additionally, our understanding of anatomy has also improved, which has contributed to modification of previously used techniques.
When injecting, optimal outcomes will result when anatomy guides the practitioner. When injecting the glabella, the procerus determines the position of the medial eyebrow as it is an eyebrow depressor [ ]. Injecting this muscle too high may result in targeting fibers of the frontalis and result in a medial brow ptosis [ ]. Common teachings suggest injecting both the medial and lateral components of the corrugator supercilli muscles; however, injecting the lateral portion of the muscle can also result in eyebrow ptosis by inadvertently injecting the elevating fibers of the frontalis [ ]. By only injecting the medial portion of the corrugator at its bony origin, the risk of ptosis is limited and the desired elevation effect is achieved [ ].
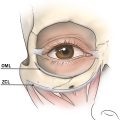
The frontalis is the only eyebrow elevating muscle [ ]. Injecting the lower forehead can risk causing an eyebrow ptosis [ ]. Cotofana and colleagues illustrated that the frontalis has bidirectional movement, the lower forehead moves cranially and acts as an eyebrow elevator, and the upper forehead moves caudally acting as a hairline depressor on contraction [ ]. Between this bidirectional movement is an immobile zone called the “line of convergence” [ ]. Practitioners can use this anatomic feature to optimize results by limiting injections of the frontalis to above the line of convergence and/or reducing neuromodulator dosing when extending the injection pattern below the line of convergence [ ]. Depth of injection of the frontalis can also contribute to the risk of a brow ptosis. By keeping injections superficial, in the superficial fatty layer above the frontalis, below the line of convergence, the risk of brow ptosis is reduced while also reducing the horizontal rhytides giving patients the results they desire [ ].
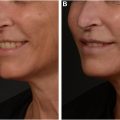
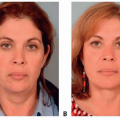
Facial biomechanics focuses on how facial soft tissue moves and its affect during animation and aging [ ]. This concept can be applied when using neuromodulators in the lower face to affect the upper face. It has been demonstrated that injecting the depressor anguli oris (DAO) as well as the superficial component of the platysma muscle at 3 points 1 cm superior to the mandible going toward the ear lobe can improve the infraorbital hallows [ ]. This same technique was previously demonstrated to increase midface volume and decrease lower face volume [ ]. The concept behind this biomechanical technique is relaxation of the platysma muscle, which is a depressor, thereby allowing facial elevating muscles such as the zygomaticus major and minor, among others, to lift [ ].
Technique
- •
When treating glabellar lines in a 3-point injection technique, the procerus muscle should be injected with a single injection point down to bone at the level of the line between the medial canthal ligaments, midline of the nasal bone [ ]. The medial corrugator muscles are injected at the medial and inferior margin of the eyebrow, also down to bone [ ]. The lateral corrugators are not injected [ ].
- •
Consider not only injecting the upper frontalis deep in the muscle and more superficially in the lower portions of the frontalis to optimize reduction of rhytides but also reducing the risk of ptosis [ , ].
Clinical pearls and potential adverse events
- •
Let the patient’s anatomy guide the injection pattern. Aim to target muscle origins. When treating glabellar lines, avoid injecting above the hairy eyebrow to avoid inadvertently injecting the frontalis [ ].
- •
Neuromodulator injected more superficially will not last as long as injected in muscle; remember to educate patients on the duration of effect.
- •
Expert knowledge of lower face musculature is necessary when performing injections of the platysma and DAO muscles. Ensure injections are away from the depressor labii inferioris and risorius muscles to prevent an asymmetric smile. Spread of effect of the chosen neuromodulator, impacted by dilution and botulinumtoxin choice, is imperative to ensure minimal adverse effects [ ].
Off-face treatments
Treating anatomic areas off the face and neck with neuromodulators has become increasingly popular because practitioners find new ways to use botulinumtoxins for esthetic use. One anatomic area that has recently overtaken the media is neuromodulator treatment of the trapezius muscle for contouring of the shoulder and neck area. A hypertrophic trapezius muscle can give an overly bulky and wide appearance, which is concerning to women who desire a slender, delicate, and feminine silhouette [ , ]. The origin of the trapezius muscle is at the occipital protuberance, nuchal ligament, and supraspinous ligament between the 8th and 12th thoracic vertebrae [ , ]. The muscle inserts into the lateral third of the clavicle, acromion, and spine of the scapula [ ]. This muscle helps maintain posture as well as extension of the neck, and elevation, rotation, adduction, and stabilization of the scapula [ , ]. The spinal accessory nerve is the primary motor nerve innervating this muscle [ , ].
In a small study conducted by Wang and colleagues, the investigators used ultrasonography to determine that the approximate depth from the skin surface to the middle of the trapezius muscle was approximately 0.87 to 1.29 cm; an appropriately sized needle is required to deliver a satisfactory treatment [ ]. It should be highlighted that the treatment of the trapezius muscle is off-label and that there are no established dosing guidelines backed by robust clinical studies [ ]. In one study, approximately 35 to 70 U of botulinumtoxin-a were used per side, distributed among 5 to 7 injection sites spaced approximately 1 to 2 cm apart [ ].
Other off-face areas to treat with neuromodulators that are gaining traction are the deltoid and gastrocnemius muscles for shoulder and calf contouring, respectively [ , ]. Injection of these anatomic areas is not without risk of significantly weakening muscles that are needed for activities of daily living.
Technique
- •
To help delineate the contour of the trapezius muscle, ask the patient to shrug their shoulders [ ].
- •
Ensure that injections are at least one fingerbreadth above the clavicle when injecting near the supraclavicular margin [ ].
- •
The first injection point should be approximately 2 cm medial to the intersection point between the lateral clavicle margin and the superior edge of the trapezius muscle [ ]. Point the needle medial and away from the shoulder area to ensure no diffusion of product into the deltoid muscle, which would potentially inhibit shoulder joint extension [ ].
- •
The most medial injection point is the intersection between the neck and the superior edge of the trapezius muscle [ ].
- •
About 5 to 7 injection points are usually sufficient [ ].
- •
The author prefers to take a more conservative approach and start with between 20 and 30 U per side and titrate up as needed.
Clinical pearls and potential adverse events
- •
Injecting the trapezius muscle is not without risk; there have been reports of excessive administration of neuromodulator or damage to the primary branch of the spinal accessory nerve contributing to the development of subacromial impingement syndrome [ ].
- •
Avoid using an extralong needle because the apex of the lung is only 2 to 3 cm above the medial segment of the clavicle [ ].
Improving skin quality with neuromodulators
When conducting a consultation with a patient, the one pillar of rejuvenation that should be kept front and center is overall skin quality with a focus on skin tone/coloration, texture/smoothness, and pores [ ]. Although a patient may present for concerns regarding volume loss or minute imperfections, the astute practitioner will reframe the patient’s perspective from the microscopic view to a more macro perspective—focusing on skin quality will help achieve this goal. By improving the quality of the skin, the skin in and of itself will look healthier and more vibrant by allowing light to reflect more evenly, giving a patient a radiance that is universally desired. Moreover, by improving the overall health of the skin, the result of other procedures such as dermal fillers will be optimized. There are now many modalities to improve a patient’s skin quality including recently FDA-approved skin boosters; however, neuromodulators, which are the workhorse of esthetic medicine, can be strategically used in this regard.
In a review by Beuttler and colleagues, several small studies demonstrated improvement of both sebum production as well as a reduction of pore size when neuromodulators are injected in an intradermal fashion [ , ]. The neuromodulator of choice is typically hyperdiluted and injected throughout the treatment zone [ ]. This technique is sometimes called “microbotox” or “mesobotox” [ ]. Although the exact mechanism of how botulinumtoxin-a decreases sebum production is unknown, one theory is the anticholinergic effect of botulinumtoxin blocking the stimulation of sebocytes and subsequently decreasing the oil gland’s autocrine function [ ]. The neuromodulatory effect of botulinumtoxin will also affect the arrector pili muscles [ ].
Neuromodulators can also improve facial erythema and flushing commonly seen in patients with rosacea and can help augment results achieved through typical treatment modalities such as pulsed dye lasers and intense pulsed light [ , ]. It has been shown that neuropeptides such as acetylcholine and vasoactive intestinal peptide are elevated in those who suffer from rosacea and contribute to vasodilation [ , ]. By injecting neuromodulators intradermally, there is a decrease in these neuropeptides, which decreases inflammation and vasodilation [ ]. There is evidence that neuromodulators can also reduce mast cell degranulation [ ]. In one clinical trial, there was improvement for up to 3 to 4 months [ , ].
The impact of long-term neuromodulator use improving skin pliability, elastic recoil, and overall collagen production can be appreciated by clinicians and patients alike; however, the exact mechanism behind these benefits is lacking [ ]. Small studies have demonstrated an increase in skin thickness and improved collagen organization with neuromodulator use; however, the impact of the needle pricks is a confounding variable [ , ].
Technique
There are a variety of methods of preparing a neuromodulator for intradermal injection with small aliquots. One method suggests diluting botulinumtoxin-a with 2.5 mL of saline and injecting 20 to 28 U over approximately 100 to 120 intradermal injections [ ]. However, other high-dose methods suggest injecting 3 to 6 U per aliquot spaced 1 cm apart [ ].
Clinical pearls and potential adverse events
- •
It is imperative to stay superficial and ensure the injection is truly intradermal. Inadvertently injecting intramuscularly could potentially cause facial asymmetries and unintended suboptimal cosmetic results.
To treat or not to treat during pregnancy and lactation
There has never been nor will there likely ever be a clinical trial investigating the safety of neuromodulator use in pregnant or lactating patients. However, practitioners, from time to time, are faced with the challenge of such a patient seeking cosmetic neuromodulator treatment or unknowingly pregnant patients receiving such a treatment. Knowing how to handle these quandaries will help guide the patient more effectively and ease uncertainty and anxiety.
First, current studies indicate that if neuromodulators are injected intramuscularly or intradermally, the systemic concentration of these drugs is inconsequential [ ]. In a review by Lee and colleagues, it was demonstrated that there are a few case reports in the dermatology literature demonstrating no adverse effects in either the fetus or mother when neuromodulators were administered for cosmetic reasons to unaware pregnant patients [ ]. There are many more reports in the neurology literature demonstrating the use of neuromodulators for therapeutic use, for a variety of conditions including cervical dystonia and migraines, in pregnant patients who had normal pregnancies [ , ]. Additionally, some reports even followed the children of treated mothers, which demonstrated normal development through 5 years of follow-up [ ]. There are rare reports in the literature of fetal demise following neuromodulator treatment of pregnant mothers; however, in all cases, these mothers had a prior history of miscarriages and so no absolute causation could be determined [ ]. Additionally, it needs to be highlighted that botulinumtoxin-a is a large molecular weight molecule and is unlikely to pass through the placenta [ , ]. Additionally, the doses of neuromodulators for cosmetic use are typically considerably lower than those used for therapeutic use, potentially alleviating the risk even further [ ].
Clinics care points
- •
The patient should be thoroughly informed about all reported and theoretic risks associated with undergoing an elective, nonessential, enhancement procedure while pregnant or lactating [ ]. Highlight that neuromodulators have not been thoroughly studied in this patient population and such a treatment is considered off-label.
- •
Lactating patients pose an interesting conundrum. The often, and quite frankly easy, recommendation often proposed to this patient cohort is to “pump and dump” for a specified period of time postprocedure. This technique may seem easy; however, for individuals who produce an inadequate supply of breast milk this may be a difficult and unrealistic recommendation to comply with.
- •
A more reasonable approach is for the patient to pump as normal; however, add the newly pumped milk postprocedure to previously stored milk for the next specified period. This can alleviate angst about wasting milk supply as well as essentially diluting out the postprocedure pumped milk. It should be clear that this technique is not recommended for procedures that involve drugs that are known to pass through breast milk.
Related posts:
 Festoon Evaluation and Management
Festoon Evaluation and Management
 Daxxify: Recommendations for Treatment
Daxxify: Recommendations for Treatment
 Nonsurgical Approach for Neck Rejuvenation
Nonsurgical Approach for Neck Rejuvenation
 Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 Indications and Technique for Extended SMAS Face-Lift and Necklift
Indications and Technique for Extended SMAS Face-Lift and Necklift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


