Application of dorsal preservation rhinoplasty techniques requires an in-depth understanding of the underlying nasal anatomy. A key tenant of dorsal preservation rhinoplasty is maintaining the relationship between the upper lateral cartilages and nasal bones. In this study, the authors discuss the pertinent nasal anatomy, surgical approaches to the nasal septum and bony pyramid, management of blocking points, and fixation of the lowered dorsum. They also introduce a new dorsal fixation method termed the “dorsal osseocartilaginous horizontal mattress” suture developed by the senior author for application in cases of combined structural and open dorsal preservation rhinoplasty.
Key points
- •
Detailed understanding of the relevant nasal anatomy is important for the application of dorsal preservation rhinoplasty.
- •
Dorsal hump reduction using preservation techniques requires manipulation of the underlying septum and bony nasal pyramid.
- •
Identification of anatomic blocking points that prevent dorsal extension and impaction is a key surgical step.
- •
Fixation of the dorsum into its new lowered position is important to counteract tensile forces that could lead to dorsal hump recurrence.
- •
The dorsal flattening suture is introduced as a novel technique to assist in combining open dorsal preservation rhinoplasty with modified extracorporeal septoplasty techniques.
Introduction
Preservation rhinoplasty is a surgical approach focused on reshaping the nose without disrupting native dorsal esthetic lines, nasal ligaments, soft tissue skin envelope, muscle attachments, and limiting excision of alar cartilages. Preservation of nasal ligaments and the soft tissue skin envelope is achieved through a subperichondrial–subperiosteal dissection. The maintenance of the bony-cartilaginous dorsum without violation of the osseocartilaginous interface is the goal of dorsal preservation rhinoplasty (DPR) and can be performed with or without disruption of the nasal soft tissues. The DPR technique and tip rhinoplasty are made more accessible through an open approach as it provides direct visualization of the entire nasal framework and is the preferred method for “structural preservation” rhinoplasty approaches.
Open structural rhinoplasty with Joseph or conventional hump reduction (CHR) techniques remains the predominate approach to rhinoplasty teaching and practice. However, the surgeon must attend to iatrogenic deformities that result from these procedures. An original advantage of DPR over conventional dorsal hump reduction techniques is the opportunity to achieve a more natural esthetic and functional result by avoiding disruption of the dorsal keystone area and osseocartilaginous vault. With adoption of some bony surface modification techniques, the primacy of preservation of the cartilaginous vault has become most fundamental. Ultimately, dorsal preservation techniques have 2 related components: approaches to the bony nasal pyramid and management of the septum. The reader may find it useful to conceptualize and compare the movements of the osseocartilaginous vault in CHR (medial) with DPR (extension/flattening and impaction). The goal of this study is to highlight pertinent nasal anatomy as it applies to the biomechanics underlying DPR.
Anatomy of dorsal preservation rhinoplasty
Nasal Septum and Upper Lateral Cartilages
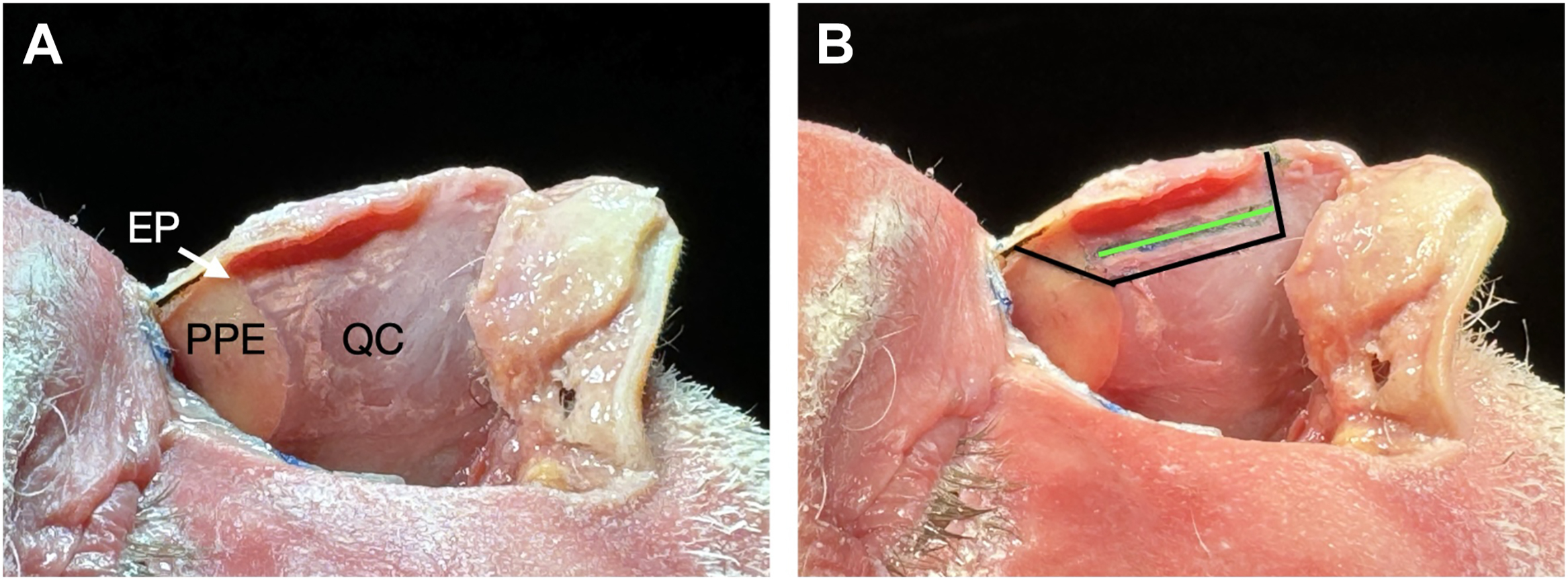
The nasal septum is a midline structure composed of hyaline cartilage anteriorly and bone posteriorly. The bony septum is formed by 4 bones: the vomer, perpendicular plate of the ethmoid (PPE), the maxillary, and the palatine bone. The maxillary and palatine bones form the septal crest. The attachment of the upper lateral cartilages (ULCs) to the undersurface of the nasal bone and cartilaginous septum at the midline is known as the dorsal keystone area (DKA). , Extension of the ULCs under the lateral portion of the nasal bones makes up the lateral keystone area (LKA). The quadrangular cartilage (QC) is securely attached to the ethmoid and vomer posteriorly maxillary crest and anterior nasal spine inferiorly. , The ethmoid point is the location where the PPE joins the QC on the undersurface of the nasal bones and in the majority of cases is located more proximal to the dorsal hump ( Fig. 1 ).
In DPR, the DKA and LKA are preserved. The overlap of the nasal bones and ULC at the keystone area is variable with anatomists reporting an average length of approximately 9 mm. , A key variable in this area for DPR is the fusion of the perichondrium of the cartilaginous vault with the periosteum of the nasal bones over the dorsum which makes this junction flexible. Additionally, the extension of the cartilaginous septum and ULCs underneath the nasal bones is a major tenant of DPR because the bony cap sits above cartilage and not septal bone. Therefore, dorsal hump descent can occur via removal of a cartilaginous strip with minimal or no subdorsal septal bone removal. The dorsum will descend from a point cephalic to the DKA and result in a lowering effect of the dorsum as well as increased rotation at the anterior aspect of the septum and nasal tip due to the flexible bony-cartilaginous connection at the dorsum.
Nasal Bones
The attachment of the nasal bones to the frontal bone corresponds with the radix or nasal root. The radix angle is obtuse with variations in values and position with gender. In female individuals, it tends to lie at the level of the upper lashes, while in male individuals, it is at the level of the superior tarsal crease and is less obtuse. The nasal profile demonstrates 4 key anatomic points for the nasal bones: (1) the nasion is the midpoint of the nasofrontal suture line; (2) the sellion is the deepest depression of the nasal bones; (3) the kyphion is the most prominent point of the bony dorsum; and (4) the rhinion is the most caudal point of the nasal bones. There are 2 major configurations to the nasal bones: S shaped and V shaped. The S-shaped nasal bones have a curve that begins at the sellion with an apex at the kyphion and plateaus at the rhinion. The V-shaped nasal bones have a nearly straight configuration from the sellion through the rhinion. In DPR, the nasal vault is pushed inferiorly; the kyphion is not resected. Therefore, patients with S-shaped nasal bones may be at a higher risk of a residual hump. The nasal bones attach to the ascending maxillary processes laterally. It is important to preserve the attachment of the medial canthal tendons to the ascending processes of the maxilla when performing wedge otectomies or lateral osteotomies.
Surgical approaches to dorsal preservation rhinoplasty
Osteotomies
A key principle of DPR is maintenance of the bony nasal vault and associated dorsal esthetic lines. Currently, there are 2 approaches that allow for lowering of the dorsum: pushdown and letdown. The pushdown technique was first described by Goodale , and popularized by Cottle and Loring. It involves single bilateral lateral and transverse osteotomies resulting in disarticulation of the nasal-frontal junction and impacting the nasal pyramid into the pyriform aperture. The letdown technique was first described in 1914 by Lothrop and involves both transverse and lateral osteotomies as well as resection of bilateral bony wedges along the ascending process of the maxilla. Thereby, lowering the nasal pyramid to rest on the maxilla instead of into the nasal cavity. A limitation of the pushdown technique is the inferior turbinate’s attachment to the lateral nasal sidewall. Therefore, the letdown technique has the advantage of lowering dorsal humps that are greater than 4 mm. Additionally, it has been shown that the pushdown can cause internal valve narrowing due to medialization of the bones, whereas the letdown preserves the nasal valve. Yet another advantage of the letdown over the pushdown is its application to the crooked nose. Removal of asymmetric wedges of bone between the 2 sides will shift the entire bony pyramid and avoid exposure of challenging high septal deviations.
Septal Excision
Regardless of which osteotomy approach is used, the bony-cartilaginous relationship of the dorsum requires some form of septal excision or manipulation to achieve dorsal hump lowering. Multiple approaches to the septum have been described in DPR with the main differentiating factor between each being the location of the septal cartilage excision. These include subdorsal excision (Saban method), inferior septal excision (Cottle method), subdorsal Z-flap, tetris concept, and modified subdorsal strip method (MSSM) developed by the senior author (S.P.M.).
Subdorsal septal excision
In Goodale’s original description of his dorsal preservation technique, he removed a segment of cartilage immediately under the dorsum with a pushdown procedure. , Lothrop also described using a subdorsal cartilage resection in combination with a letdown procedure to achieve the dorsal hump reduction. The approach was also utilized by the early modern adopters of DPR including Gola and then Saban. The technique involves making an incision along the contour of the dorsal hump immediately under the dorsum and extending it to the anterior septal angle. Minimal to no septal cartilage remains superior to this incision. A more inferior cut is made at a location several millimeters below the dorsal cut. The segment of cartilage between these 2 incisions is removed and represents the amount of dorsal reduction. , A portion of the PPE is also resected in this method to allow for successful descent of the dorsum. If any cartilage remains under the dorsum, it is scored to release tension that may prevent flattening. The dorsum is then sutured to the underlying septum in its lowered position. Advocates for this approach tout the control in the design of the lower incision and thereby the corresponding intended contour of the nasal profile.
Inferior septal excision
Cottle and Loring first applied excision of septal cartilage from the premaxilla in the setting of nasal fractures to allow for mobilization after down-fracture of the nasal bones. They then translated this technique to rhinoplasty and found that resection of a strip of cartilage at the maxillary spine allowed for descent of the dorsum. The amount of cartilage removed corresponds to the observed dorsal reduction. To facilitated complete removal of the dorsal hump, the inferior cartilage excision is combined with resection of a vertical 4 mm segment at the bony cartilaginous junction and resection of PPE under the nasal bone. The remaining cartilage and dorsum are then stabilized into position with sutures. The disadvantages of this approach include the complexity of the cartilage cuts and the degree of difficulty associated with anchoring the septal cartilage to the nasal spine.
Subdorsal Z-flap
Kovacevic and colleagues describe a modification to the inferior septal excision by combining it with the high septal strip approach. The technique involves making a vertical subdorsal cartilaginous septal incision at the highest point of the corresponding dorsal hump. Then, a 30° angled cut is extended from the caudal end of the septal junction with the ULC (W-point) to create a triangular-shaped incision that meets the vertical incision. Lastly, a subdorsal resection just below the bony hump is completed connecting the vertical septal cut with the median radix osteotomy. The dorsum is then secured in its new position with sutures. The authors advocate its use in V-shaped and S-shaped humps and noses with axis deviations.
Tetris concept
The tetris concept was developed by Neves and colleagues as a modification of the midseptal excision. The midseptal excision technique had been advocated for by Ishida, Neves, and their colleagues , for its ability to lower the cartilaginous nasal vault. The excision starts from the bony-cartilaginous junction and extends anteriorly into the caudal aspect of the septum inferior to the anterior septal angle. However, a limitation with this technique arose in that the caudal border of the septum often needed to be stabilized to prevent lateralization. Therefore, Neves and colleagues described the tetris concept that involves maintaining a caudal strut and rectangular subdorsal strip while excising a midseptal strip of cartilage and triangular wedge of bony septum under the nasal bones. The result is flattening of the dorsum while leaving the caudal strut intact.
Modified subdorsal strip method
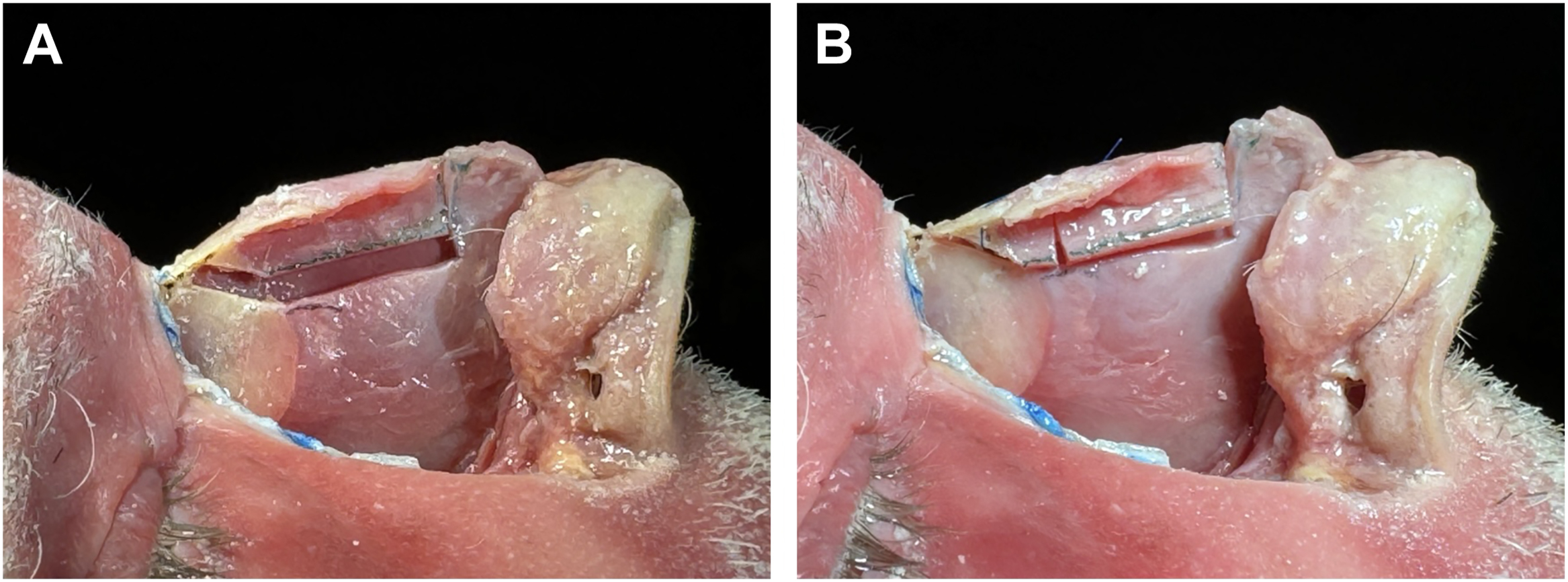
The MSSM was developed by the senior author (S.P.M.) as an intermediate between the classic subdorsal and inferior septal resections. Similar to the tetris concept, the approach involves maintaining a 3 mm to 5 mm subdorsal strip of cartilage and incising parallel to the dorsum from the bony cartilaginous junction toward the caudal septum terminating posterior to the anterior septal angle (see Fig. 1 ). Therefore, a 1 cm to 1.5 cm strut of caudal septal cartilage is maintained. The paraseptal cleft of fibrous attachments between the ULC at the anterior septum is released to allow for improved visualization of the septum and unimpeded dorsal descent. An advantage of the remaining caudal strut of septum is the freedom to attach the tripod complex in any desired projected or rotated position. While a triangular segment of ethmoid bone is commonly removed in other techniques, the senior author prefers to create a longitudinal cut into the bony septum such that there is slight side-to-side overlap between bones once the dorsum is lowered ( Fig. 2 ). This conservative approach to the bony septum aims to minimize over displacement of the disarticulated nasal vault into the nose. Additional advantages of this method compared to others include the ability to resect lower and posterior septum and the caudal strut remains in continuity with the maxillary spine ( Fig. 3 ). As such, septal deviations are corrected, additional cartilage is harvested for grafting purposes and there is no need to stabilize the septum to bone.