This article concentrates on the less-common cutaneous malignancies such as merkel cell, atypical fibroxanthoma, malignant fibrous histiocytoma, dermatofibrosarcoma protuberans, microcystic adnexal carcinoma, and sebaceous carcinoma. The clinical and histopathologic descriptions of each, most current and emerging etiologies, diagnosis, staging, treatment, and prognosis are discussed.
- •
In what was once a disease of older generations, the overall incidence of cutaneous malignancies continues to increase, with a disproportionate increase in younger patients likely as a result of increasing sun exposure.
- •
UVB rays cause most damage associated with carcinogenesis, as a consequence of energy absorption in different skin layers. UVA rays penetrate deeper into the dermis resulting in solar elastosis, whereas UVB rays are almost completely absorbed by the epidermis.
- •
Public education is the first step in curbing the increase in potentially preventable neoplasms.
Introduction
The lifetime risk for any American to develop some form of skin cancer has been estimated to be one in five. A large proportion of these cutaneous malignancies fall into the category of nonmelanoma skin cancer with malignant melanoma comprising a smaller proportion. Incidence of nonmelanoma skin cancer has been reported to be 18 to 20 times greater than that of malignant melanoma. Within the category of nonmelanoma skin cancer, the ratio of basal cell carcinoma to squamous cell carcinoma is approximately 4:1. In what was formerly a disease of older generations, the overall incidence of these malignancies continues to increase, with a disproportionate increase in younger patients likely caused by increasing sun exposure.
Ultraviolet (UV) radiation exposure is a significant inciting or contributing factor in almost all cutaneous malignancies. Within the UV spectrum, it has been shown that UVB rays (290–320 nm) cause most damage associated with carcinogenesis, whereas UVA rays (320–400 nm) contribute to overall age-related changes in the skin. This is partly caused by the site of energy absorption in different skin layers. UVA rays penetrate deeper into the dermis resulting in solar elastosis, whereas UVB rays are almost completely absorbed by the epidermis. The absorption of UVA radiation also is predominantly by non-DNA chromophores, leading to indirect DNA damage through the creation of reactive oxygen species causing single strand breaks. This is less traumatic than UVB radiation causing direct DNA damage through dimer formation. The primary process responsible for repair of damaged DNA is the nucleotide excision repair mechanism. If this mechanism is overwhelmed, usually through continuous or repeated UV exposure, the damage goes unrepaired. When these mutations affect genes encoding regulatory functions, uncontrolled proliferation occurs. The most well-studied mutation is with the p53 tumor suppressor gene.
Basal cell carcinoma and squamous cell carcinoma comprise most nonmelanoma skin cancers. Other histologic forms, such as Merkel cell carcinoma (MCC), atypical fibroxanthoma (AFX), malignant fibrous histiocytoma (MFH), dermatofibrosarcoma protuberans (DFSP), microcystic adnexal carcinoma (MAC), and sebaceous carcinoma, are also described in this category, although their incidence is much lower. There is abundant information in the literature on basal cell carcinoma and squamous cell carcinoma. This article concentrates on the less-common malignancies.
MCC
MCC is a relatively new tumor, previously called trabecular carcinoma or cutaneous neuroendocrine carcinoma. The Merkel cell is the only cutaneous cell known to contain neurosecretory granules and resides in the basal layer of the epidermis. There is still debate as to whether the Merkel cell is of neuroendocrine origin or a puripotent stem cell. Even the function of these cells remains to be fully understood, although they are thought to play a role in mechanoreception and endocrine signaling. They do, however, form a very small but aggressive portion of the nonmelanoma skin cancers.
The incidence of MCC in the United States is estimated to be between 0.32 and 0.44 per 100,000 person-years. Males have a higher incidence than females at approximately 2:1, and whites have approximately eight times the risk of blacks. MCC is rare in persons younger than age 50 years, then increases between ages 50 and 65. Like other nonmelanoma skin cancers, the incidence increases in areas of higher UV exposure, with the most common location being on the head and neck (48%), upper limb (19%), lower limb (16%), and trunk (11%).
The cause of MCC has not been completely elucidated. Many contributing factors are being suggested and trends have been observed, but no definitive factors have been reported. MCC has been seen in many forms of immunosuppression, both autoimmune and iatrogenic. There have been reports of partial regression of metastatic lesions after discontinuation of immunosuppression. This risk is not specific to MCC, because the risks of other malignancies also increase with any degree of immunosuppression.
UV radiation is strongly associated with the development of MCC. Although no conclusive evidence has shown causation, their occurrence within a background of solar elastosis, Actinic keratoses, and other UV-induced changes strongly suggests a contributing effect. Mutations in the p53 tumor suppressor gene have also been identified in MCC, a change considered diagnostic of UV-induced DNA damage. Patients with psoriasis undergoing psoralen-UVA therapy have shown a 100-fold increase over the general population in incidence of MCC, indicating UVA along with UVB radiation plays a role.
Viral infection has been the most studied and promising etiologic factor. Recently, Feng and colleagues characterized a new polyomavirus, Merkel cell polyomavirus. Approximately 80% of individuals older than 50 years show seropositivity to Merkel cell polyomavirus, although little is known about transmission and latency. Since this discovery, many groups have published data on prevalence of Merkel cell polyomavirus DNA in MCC lesions, with rates ranging from 40% to 100%. Further research is needed to determine the virus’ role in carcinogenesis.
Commonly, MCC develops as an asymptomatic rapidly growing nodule (over 6–12 months). The tumor is usually flesh colored, firm, and nontender. There may be overlying telangiectasia and the differential diagnosis may include a simple cyst, basal cell carcinoma, adnexal tumor, amelanotic melanoma, or other nondescript cutaneous lesion. Diagnosis is established by biopsy ( Fig. 1 ).
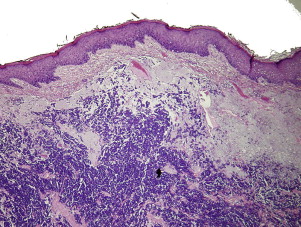
Immunohistochemistry is important in the diagnosis, because the histopathology can be similar to other cutaneous malignancies. MCC is positive for epithelial (CK20) and neuroendocrine (NFP) markers, whereas lacking markers for lymphoid or melanoma lesions.
Since its description, multiple staging systems have been discussed. Only recently, a single system has emerged and gained universal acceptance. This staging system was recently published by the American Joint Committee on Cancer in their 7th edition, 2010 version, and maintains the standard T1 to T4 categories ( Tables 1 and 2 ).
| T | N | M |
|---|---|---|
| Tx – primary tumor cannot be assessed | Nx – regional nodes cannot be assessed | Mx – distant metastasis cannot be assessed |
| T0 – no primary tumor | N0 – no regional node metastasis | M0 – no distant metastasis |
| Tis – in situ primary tumor | cN0 – nodes not clinically detectable | M1 – distant metastasis |
| T1 – primary tumor ≤2 cm | cN1 – nodes clinically detectable | M1a – distant skin, distant subcutaneous tissue, or distant lymph node metastasis |
| T2 – primary tumor ≥2 cm but ≤5 cm | pN0 – nodes negative by pathologic evaluation | M1b – lung metastasis |
| T3 – primary tumor >5 cm | pNx – nodes not evaluated pathologically | M1c – metastasis to all other visceral sites |
| T4 – primary tumor invades bone, muscle, fascia, or cartilage | N1a – micrometastasis | |
| N1b – macrometastasis | ||
| N2 – in-transit metastasis |
| Stage | Stage Grouping | ||
|---|---|---|---|
| 0 | Tis | N0 | M0 |
| IA | T1 | pN0 | M0 |
| IB | T1 | cN0 | M0 |
| IIA | T2/T3 | pN0 | M0 |
| IIB | T2/T3 | cN0 | M0 |
| IIC | T4 | N0 | M0 |
| IIIA | Any T | N1a | M0 |
| IIIB | Any T | N1b/N2 | M0 |
| IV | Any T | Any N | M1 |
Recurrence rates have been reported from 25% to 30%, regional lymph node involvement in 52% to 59%, and distant metastasis in 34% to 36% of all MCC. This tumor carries a higher metastatic and mortality rate than malignant melanoma, so the treatment algorithm is much more aggressive.
Surgery is the primary treatment modality for MCC, although there is still debate on adjuvant therapy after resection. The current National Comprehensive Cancer Network guidelines support the use of wide local excision with 1- to 2-cm margins or Mohs micrographic excision. Further treatment depends on involvement of primary lymph node drainage basins. Because of the high rate of lymph node involvement, sentinel lymph node biopsy is recommended. Approximately one-third of patients are understaged if this is not done because of occult microscopic nodal involvement. If sentinel lymph node biopsy is positive, completion neck dissection or radiation therapy is indicated. The use of radiation therapy after excision has been shown to improve local and regional recurrence rates. Radiation therapy alone has demonstrated control rates in 75% of primary lesions. Either primary or adjuvant chemotherapy has been used mainly for metastatic disease, but no survival benefit seems to be gained by its use.
The overall 5-year survival of MCC is around 62%. The 5-year survival rate for patients with local disease only is 64%, whereas survival for patients with nodal disease and distant metastasis decreases to 39% and 18%, respectively. This low survival for local disease is largely caused by the discrepancy between T1 lesions (stage IA, 79% 5-year survival) and T4 lesions (stage IIC, 47% 5-year survival), which both fall into this category. Primary lesions on the upper limb and younger age are independently associated with a better prognosis.
A mucosal variant is also seen but at a much lower incidence. The most commonly affected site is the larynx, followed by nasal cavity, pharynx, and the mouth and tongue. This has a much poorer prognosis than cutaneous MCC with the overall survival rate being 49% at 2 years.
MCC
MCC is a relatively new tumor, previously called trabecular carcinoma or cutaneous neuroendocrine carcinoma. The Merkel cell is the only cutaneous cell known to contain neurosecretory granules and resides in the basal layer of the epidermis. There is still debate as to whether the Merkel cell is of neuroendocrine origin or a puripotent stem cell. Even the function of these cells remains to be fully understood, although they are thought to play a role in mechanoreception and endocrine signaling. They do, however, form a very small but aggressive portion of the nonmelanoma skin cancers.
The incidence of MCC in the United States is estimated to be between 0.32 and 0.44 per 100,000 person-years. Males have a higher incidence than females at approximately 2:1, and whites have approximately eight times the risk of blacks. MCC is rare in persons younger than age 50 years, then increases between ages 50 and 65. Like other nonmelanoma skin cancers, the incidence increases in areas of higher UV exposure, with the most common location being on the head and neck (48%), upper limb (19%), lower limb (16%), and trunk (11%).
The cause of MCC has not been completely elucidated. Many contributing factors are being suggested and trends have been observed, but no definitive factors have been reported. MCC has been seen in many forms of immunosuppression, both autoimmune and iatrogenic. There have been reports of partial regression of metastatic lesions after discontinuation of immunosuppression. This risk is not specific to MCC, because the risks of other malignancies also increase with any degree of immunosuppression.
UV radiation is strongly associated with the development of MCC. Although no conclusive evidence has shown causation, their occurrence within a background of solar elastosis, Actinic keratoses, and other UV-induced changes strongly suggests a contributing effect. Mutations in the p53 tumor suppressor gene have also been identified in MCC, a change considered diagnostic of UV-induced DNA damage. Patients with psoriasis undergoing psoralen-UVA therapy have shown a 100-fold increase over the general population in incidence of MCC, indicating UVA along with UVB radiation plays a role.
Viral infection has been the most studied and promising etiologic factor. Recently, Feng and colleagues characterized a new polyomavirus, Merkel cell polyomavirus. Approximately 80% of individuals older than 50 years show seropositivity to Merkel cell polyomavirus, although little is known about transmission and latency. Since this discovery, many groups have published data on prevalence of Merkel cell polyomavirus DNA in MCC lesions, with rates ranging from 40% to 100%. Further research is needed to determine the virus’ role in carcinogenesis.
Commonly, MCC develops as an asymptomatic rapidly growing nodule (over 6–12 months). The tumor is usually flesh colored, firm, and nontender. There may be overlying telangiectasia and the differential diagnosis may include a simple cyst, basal cell carcinoma, adnexal tumor, amelanotic melanoma, or other nondescript cutaneous lesion. Diagnosis is established by biopsy ( Fig. 1 ).
Immunohistochemistry is important in the diagnosis, because the histopathology can be similar to other cutaneous malignancies. MCC is positive for epithelial (CK20) and neuroendocrine (NFP) markers, whereas lacking markers for lymphoid or melanoma lesions.
Since its description, multiple staging systems have been discussed. Only recently, a single system has emerged and gained universal acceptance. This staging system was recently published by the American Joint Committee on Cancer in their 7th edition, 2010 version, and maintains the standard T1 to T4 categories ( Tables 1 and 2 ).
| T | N | M |
|---|---|---|
| Tx – primary tumor cannot be assessed | Nx – regional nodes cannot be assessed | Mx – distant metastasis cannot be assessed |
| T0 – no primary tumor | N0 – no regional node metastasis | M0 – no distant metastasis |
| Tis – in situ primary tumor | cN0 – nodes not clinically detectable | M1 – distant metastasis |
| T1 – primary tumor ≤2 cm | cN1 – nodes clinically detectable | M1a – distant skin, distant subcutaneous tissue, or distant lymph node metastasis |
| T2 – primary tumor ≥2 cm but ≤5 cm | pN0 – nodes negative by pathologic evaluation | M1b – lung metastasis |
| T3 – primary tumor >5 cm | pNx – nodes not evaluated pathologically | M1c – metastasis to all other visceral sites |
| T4 – primary tumor invades bone, muscle, fascia, or cartilage | N1a – micrometastasis | |
| N1b – macrometastasis | ||
| N2 – in-transit metastasis |
| Stage | Stage Grouping | ||
|---|---|---|---|
| 0 | Tis | N0 | M0 |
| IA | T1 | pN0 | M0 |
| IB | T1 | cN0 | M0 |
| IIA | T2/T3 | pN0 | M0 |
| IIB | T2/T3 | cN0 | M0 |
| IIC | T4 | N0 | M0 |
| IIIA | Any T | N1a | M0 |
| IIIB | Any T | N1b/N2 | M0 |
| IV | Any T | Any N | M1 |
Recurrence rates have been reported from 25% to 30%, regional lymph node involvement in 52% to 59%, and distant metastasis in 34% to 36% of all MCC. This tumor carries a higher metastatic and mortality rate than malignant melanoma, so the treatment algorithm is much more aggressive.
Surgery is the primary treatment modality for MCC, although there is still debate on adjuvant therapy after resection. The current National Comprehensive Cancer Network guidelines support the use of wide local excision with 1- to 2-cm margins or Mohs micrographic excision. Further treatment depends on involvement of primary lymph node drainage basins. Because of the high rate of lymph node involvement, sentinel lymph node biopsy is recommended. Approximately one-third of patients are understaged if this is not done because of occult microscopic nodal involvement. If sentinel lymph node biopsy is positive, completion neck dissection or radiation therapy is indicated. The use of radiation therapy after excision has been shown to improve local and regional recurrence rates. Radiation therapy alone has demonstrated control rates in 75% of primary lesions. Either primary or adjuvant chemotherapy has been used mainly for metastatic disease, but no survival benefit seems to be gained by its use.
The overall 5-year survival of MCC is around 62%. The 5-year survival rate for patients with local disease only is 64%, whereas survival for patients with nodal disease and distant metastasis decreases to 39% and 18%, respectively. This low survival for local disease is largely caused by the discrepancy between T1 lesions (stage IA, 79% 5-year survival) and T4 lesions (stage IIC, 47% 5-year survival), which both fall into this category. Primary lesions on the upper limb and younger age are independently associated with a better prognosis.
A mucosal variant is also seen but at a much lower incidence. The most commonly affected site is the larynx, followed by nasal cavity, pharynx, and the mouth and tongue. This has a much poorer prognosis than cutaneous MCC with the overall survival rate being 49% at 2 years.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


