86
Ulcers
• The most common types of leg ulcers – venous, arterial, and neuropathic – as well as pressure ulcers, lymphedema, and an approach to wound healing are reviewed (see below); additional physical, inflammatory, infectious, metabolic, and neoplastic causes of leg ulcers are outlined in Fig. 86.1.
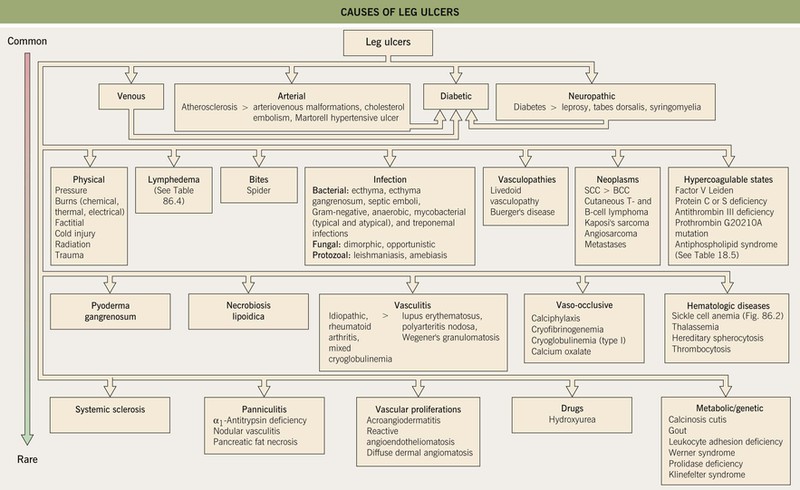
Fig. 86.1 Causes of leg ulcers. Patients with Behçet’s disease can also develop leg ulcers due to vasculitis and/or venous insufficiency related to deep vein thromboses. Erosive pustular dermatosis is another occasional cause of leg ulcers. Hydroxyurea-induced leg ulcers are exceedingly painful, surrounded by atrophic skin, and often located on the malleolus or tibial crest.
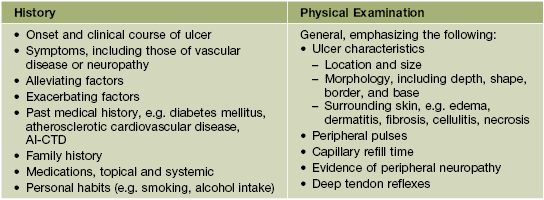
• Features to consider in the history and physical examination of patients with a leg ulcer are presented in Table 86.1, and routine laboratory testing often includes a CBC, ESR, and blood glucose and serum albumin levels; microbial cultures, evaluation for hypercoagulability (see Table 18.5), and additional studies depend on the clinical setting.
Venous Ulcers
• Venous hypertension and insufficiency represent the most common causes of chronic leg ulcers.
• Prevalence increases with age, and risk factors include female sex, obesity, pregnancy, prolonged standing, and family history of venous insufficiency; hypercoagulability can be a contributing factor, especially in patients with a history of deep vein thrombosis or livedoid vasculopathy (Fig. 86.3; see Chapter 18).


Fig. 86.3 Livedoid vasculopathy. A Multiple hemorrhagic crusts and small, very painful ulcers associated with brown discoloration due to hemosiderin deposits. B Stellate, porcelain-white atrophic scars with peripheral telangiectatic papules, referred to as atrophie blanche. B, Courtesy, Julie V. Schaffer, MD.
• Ulcers tend to have irregular borders and a yellow fibrinous base, with a predilection for the area above the medial malleolus

(Fig. 86.4); the ulcers can become large but are often fairly shallow, with granulation tissue evident upon debridement.


Fig. 86.4 Venous ulcers over the medial malleolus. A Granulation tissue is evident in ~15% of the ulcer bed. Note the surrounding stasis dermatitis with erythema, crusting, and scaling as well as scarring. B Induration due to lipodermatosclerosis, hemosiderin deposition, and atrophie blanche scars are present in the surrounding skin. B, Courtesy, Jean L. Bolognia, MD.
• Surrounding skin has signs of venous hypertension such as yellow-brown discoloration due to hemosiderin deposits, pinpoint petechiae, stasis dermatitis, lipodermatosclerosis, and, occasionally, acroangiodermatitis (Fig. 86.5).





Fig. 86.5 Associated findings in patients with venous hypertension and insufficiency. A Venulectasias of the instep. B Brown discoloration of the foot and ankle due to hemosiderin deposits within dermal macrophages in addition to hyperpigmentation. Note the cutoff at Wallace’s line. C Lipodermatosclerosis with violet-brown discoloration, tenderness, and induration that typically begins above the medial malleolus. D Stasis dermatitis and chronic lipodermatosclerosis with serous crusts and the ‘inverted champagne bottle’ or ‘bowling pin’ configuration. E Acroangiodermatitis (pseudo-Kaposi’s sarcoma). Violaceous plaque in a patient with venous hypertension. Histologically, these lesions can resemble Kaposi’s sarcoma. A, B, Courtesy, Jean L. Bolognia, MD; C, Courtesy, Kalman Watsky, MD. D, Courtesy, Ariela Hafner, MD, and Eli Sprecher, MD.
• Other findings include varicosities and edema > lymphedema of the lower extremities (Fig. 86.6); swelling and aching of the legs is worsened by dependency (e.g. prolonged standing) and improved by leg elevation and the use of compression therapy; other dependent sites, such as a large pannus, can develop similar clinical changes (Fig. 86.7).




• DDx: see Fig. 86.1; coexistent arterial insufficiency (see below) or uncompensated congestive heart failure should be excluded before initiating compression therapy.
• Evaluation and Rx: an approach to the patient with a chronic venous ulcer is presented in Fig. 86.8.
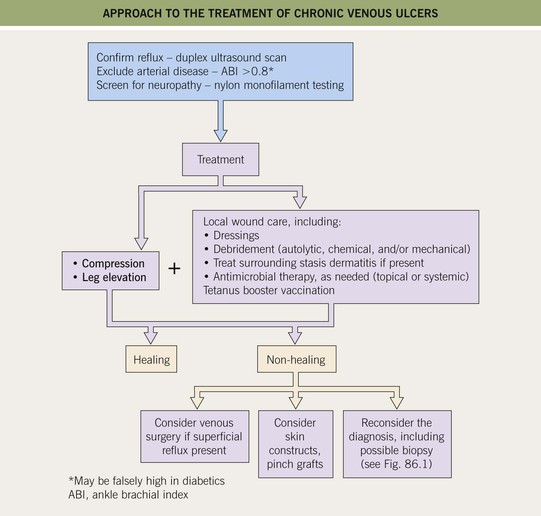
• Compression represents a mainstay of therapy.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


