39
Amyloidosis
Amyloidosis encompasses a wide range of disorders, several of which have cutaneous manifestations. The common thread is the formation of extracellular deposits that are composed of a β-pleated sheet by x-ray crystallography. In general, amyloid deposits exhibit a red color with Congo red stain and demonstrate birefringence (apple green color) under polarized light. Precursor proteins of amyloid vary from keratin to immunoglobulin (Ig) light chains to gelsolin. If necessary, tandem mass spectrometry can be performed to characterize the specific protein.
In dermatology, the initial distinction is between amyloidosis that is systemic versus skin-limited (Fig. 39.1). The former is less common than the latter.
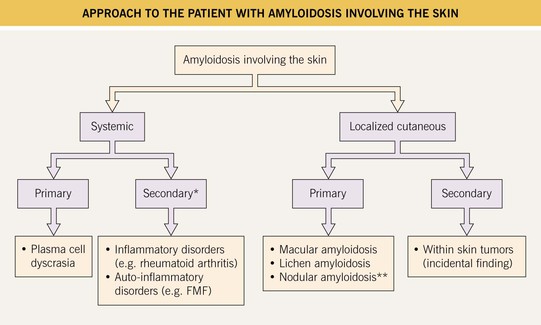
Fig. 39.1 Approach to the patient with amyloidosis involving the skin. *Cutaneous lesions are rare; **A minority of patients may develop systemic amyloidosis. FMF, familial Mediterranean fever.
Systemic Amyloidosis
• Firm skin-colored to pink to yellow-brown waxy papules or plaques occur most commonly on the face (Fig. 39.2); infiltration of the tongue can lead to macroglossia (Fig. 39.3), and occasionally there is diffuse waxy induration of the skin (sclerodermoid presentation); purpura due to trauma or pinching of the skin can also be seen and is due to the fragility of blood vessels surrounded by amyloid deposits (Fig. 39.4).

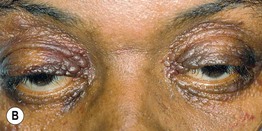
Fig. 39.2 Primary systemic amyloidosis. A Numerous waxy translucent facial papules. Some have a yellow to yellow-brown color. B Some of the waxy papules have become purpuric, but this may be difficult to appreciate because of the pigmentation of the skin; the periorbital region is a common site of involvement. A, Courtesy, Jean Bolognia, MD; B, Courtesy, Judit Stenn, MD.


Fig. 39.3 Primary systemic amyloidosis. A Macroglossia with dental impressions on the tongue. B Papulonodues of the tongue and external nares; some are purpuric while others are translucent with a yellowish hue. The combination of macroglossia plus carpal tunnel syndrome is a classic clinical presentation. B, Courtesy, Dennis Cooper, MD.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


