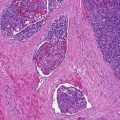
Fig. 10.1
Trichoblastic carcinoma. A large, asymmetrical lesion composed of basaloid islands with central comedo-type necrosis is adjacent to more typical-appearing trichoblastoma
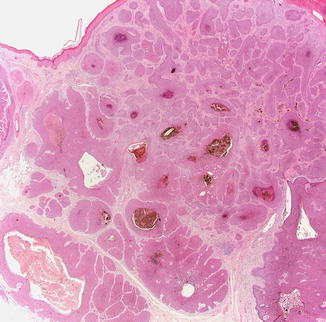
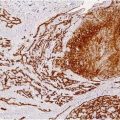
Fig. 10.2
Trichoblastic carcinoma. A deep, infiltrative, basaloid neoplasm is shown without well-developed connection to the epidermis
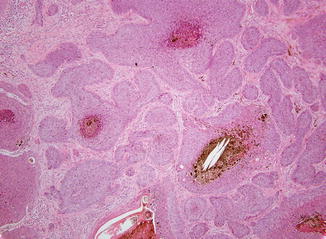
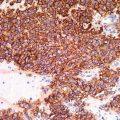
Fig. 10.3
Trichoblastic carcinoma. Basaloid tumor nests show with absence of tumor-stroma clefting, loose fibrotic stroma, and central necrosis
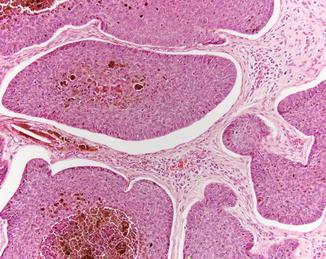
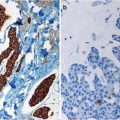
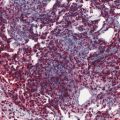
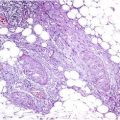
Fig. 10.4
Trichoblastic carcinoma. In some areas, epithelial islands show prominent peripheral palisading and tumor-stroma clefting, resembling basal cell carcinoma
Differential Diagnosis
The diagnosis is primarily a histological one, but clinical features such as aggressive behavior can be helpful clues. The differential diagnosis includes basal cell carcinoma, trichoblastoma, trichilemmal carcinoma, and malignant pilomatricoma (Triaridis et al. 2007). The primary features that distinguish trichoblastic carcinoma from basal cell carcinoma are the lack of peripheral palisading, lack of keratinization, nuclear pleomorphism, necrosis, and conspicuous mitoses seen in trichoblastic carcinoma. The presence of areas of benign appearing trichoblastoma merging with malignant areas is also a useful diagnostic clue. A benign trichoblastoma can be distinguished from its malignant counterpart by the lack of necrosis, cytologic atypia, and a brisk mitotic index. The neoplastic cells of trichilemmal carcinoma are clear and polygonal with peripheral palisading of cylindric cells. Malignant pilomatricoma typically demonstrate marked pleomorphism, an infiltrative growth pattern, and characteristic “ghost cells” due to aberrant keratinization (Triaridis et al. 2007).
Prognosis
Information regarding the prognosis of trichoblastic carcinoma is not readily available as the entity has been only rarely reported. Given the propensity to arise and expand deeply in the dermis, they may have a more aggressive course than basal cell carcinoma. As in other malignancies, the prognosis can be poor in the case of metastatic disease, especially in an immunocompromised patient. On the other hand, complete surgical excision can be curative.
Treatment
Complete surgical excision is the treatment of choice and is probably sufficient for the majority of tumors excised. Subsequent adjuvant radiotherapy may be useful in select cases demonstrating local aggressiveness (Laffay et al. 2012; Oufkir et al. 2013). A small study reported tyrosine kinase inhibitor therapy with sunitinib to be effective in patients with metastatic disease (Battistella et al. 2010).
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


