Scars of the cheek resulting from all causes can extol significant psychological toll. The cheek is the largest facial subunit and visually and aesthetically prominent making scars in this region difficult to ignore. An approach to scar management that targets specific characteristics of a scar using a combination of surgical and nonsurgical modalities can significantly improve the appearance of most scars. The ideal time to revise a scar should be based on the extent of scar maturation and presence or absence of any functional distortion.
Key points
- •
Scars of the cheek resulting from all causes can extol significant psychological toll.
- •
The cheek is the largest facial subunit and is visually and aesthetically prominent, making scars in this region difficult to ignore.
- •
An approach to scar management that targets specific characteristics of a scar using a combination of surgical and nonsurgical modalities can significantly improve the appearance of most scars.
- •
The ideal time to revise a scar should be based on the extent of scar maturation and presence or absence of any functional distortion.
Introduction
In times past, scars on the cheek were worn as badges of honor; signs of battle hardiness or prowess in duels. These so-called good scars were worn in a fashionable manner and did not invite negative stares. In contrast, scars resulting from traumatic events such as an assault, a dog bite, acne, or cancer treatment can have a life-long psychological impact that is more than skin deep. Studies using eye tracking have shown that the eye, nose, and lip form the central triangle of visual fixation the primary focus of most face-to-face interactions. This normal pattern of visual scan path changes significantly with attentional bias to the cheek when scars are present. The goal of scar revision is to efface the visual characteristics that attracts negative evaluation by observers and mend the adverse psychological imprints that surrounds the cause and living with the scar. An objective measure of a successful cheek scar revision will be normalization of pretreatment visual scan paths and an associated improvement in self-confidence.
In general, scars can be effaced and camouflaged but not made to vanish completely. Effacement and camouflaging are visual concepts that play on the properties of light absorption and reflection. It is therefore important to understand the physical features of a scar and their effect on visual perception when outlining a plan for scar revision. Similarly, the surface anatomy of the cheek subunits, the texture of the skin, and the underling volumetric and contour changes should be considered in treatment regimens to create a favorable cheek scar.
Introduction
In times past, scars on the cheek were worn as badges of honor; signs of battle hardiness or prowess in duels. These so-called good scars were worn in a fashionable manner and did not invite negative stares. In contrast, scars resulting from traumatic events such as an assault, a dog bite, acne, or cancer treatment can have a life-long psychological impact that is more than skin deep. Studies using eye tracking have shown that the eye, nose, and lip form the central triangle of visual fixation the primary focus of most face-to-face interactions. This normal pattern of visual scan path changes significantly with attentional bias to the cheek when scars are present. The goal of scar revision is to efface the visual characteristics that attracts negative evaluation by observers and mend the adverse psychological imprints that surrounds the cause and living with the scar. An objective measure of a successful cheek scar revision will be normalization of pretreatment visual scan paths and an associated improvement in self-confidence.
In general, scars can be effaced and camouflaged but not made to vanish completely. Effacement and camouflaging are visual concepts that play on the properties of light absorption and reflection. It is therefore important to understand the physical features of a scar and their effect on visual perception when outlining a plan for scar revision. Similarly, the surface anatomy of the cheek subunits, the texture of the skin, and the underling volumetric and contour changes should be considered in treatment regimens to create a favorable cheek scar.
Anatomic considerations
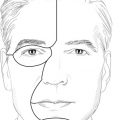
The cheek is the largest aesthetic facial subunit extending from the zygomatic arch and orbital crease superiorly to the lower border of the mandible inferiorly. Medially, the cheek is bordered by the nasofacial sulcus, and nasolabial and nasomandibular creases, and extends to the preauricular crease laterally. Based on the underlying bony skeleton and soft tissue coverage, the cheek subunit is further divided into infraorbital, zygomatic, nasolabial, buccal, and parotidomasseteric (preauricular) anatomic subunits. The thickness of the skin coverage varies across the anatomic subunits of the cheek. Skin of the infraorbital subunit is particularly thin as it transitions onto the lower eyelid. The zygomatic subunit overlies the zygomatic arch and malar prominence; the skin in this region has minimal laxity; it is fixed to the underlying fascia. The topography of the cheek transitions from a convex zygomatic subunit to a flat buccal subunit. The skin of the buccal subunit is thicker than that of the other subunits and is freely mobile over the underlying subcutaneous tissue and fascia. The parotidomasseteric subunit is the region overlying the parotid gland. The skin in this region is thinner and relatively fixed compared with that of the buccal subunit. The skin in the nasolabial subunit is thick and mobile, similar to that of the buccal subunit. The nasolabial crease is formed by direct attachment of dermis to the underlying muscles (levator labii superioris alaeque nasi and orbicularis oris) owing to the absence of the superficial musculoaponeurotic system in this area. The orientation of collagen fibers and action of the underlying muscles create relaxed skin tension lines (RSTLs) on the cheek that are curvilinear, running from the malar eminence to the inferior border of the mandible ( Fig. 1 ). Cutaneous perforators from the infraorbital, transverse facial, angular, and zygomaticofacial arteries supply the skin of the cheek.
Evaluating a patient cheek scar for revision
A detailed history of how a scar was acquired and an outline of any previous treatment are important when assessing a patient for scar revision. For example, traumatic scars allowed to heal by secondary intention may leave broad and poorly textured scars that are likely to respond well to controlled surgical repair. In contrast, a scar that has failed to improve by reexcision by an experienced surgeon may need to be approached differently because another excision is unlikely to yield significant improvement. Medical comorbidities, as far as they influence wound healing, should be considered when assessing scars for revision. A history of poor wound healing and systemic disease such as diabetes can affect the outcome of scar revision. Although individuals with darker skin tones are more prone to developing hypertrophic scarring, a patient-specific wound healing history may be more informative than a generalized skin type categorization.
The features of a scar that make it visually perceptible can direct the design and selection of a treatment modality for improving cheek scars. Cheek scars should be assessed for their color match with surrounding skin, vascularity, light reflection, texture, contour, pliability, height, relation to the RSTLs, and any distortion of the eyelid, lip, or nasal alar ( Fig. 2 ).
A wide scar may be improved by narrowing; a depressed scar that absorbs light resulting in a visible shadow is best corrected by addressing the contour discrepancy. Scars that are thick and raised may be flattened with either surgical or nonsurgical techniques and those with color and texture mismatch may be addressed with modalities that improve color and texture blend. A favorable scar is parallel to RSTLs or is hidden along the borders of aesthetic subunits. Thus, misaligned scars may be broken up and reoriented to more closely match RSTLs or repositioned into aesthetic subunit boundaries. Although preplanned surgical incisions may be placed in RSTLs, traumatic scars do not necessary respect these anatomic boundaries and may require reorienting techniques for better camouflage.
Timing of scar revision
Most scars improve with time; therefore, ample time should be allowed for healing and scar maturation before any major revision is considered. The process of scar maturation seems to be faster in patients older than 55 years old when compared with patients younger than 30 years old. The clinical macroscopic appearance of the scar, particularly the presence and progression of redness, correlates well with extent of scar maturation. Together with the patients’ age, the macroscopic appearance may be used to anticipate and plan the timing of any interventions. Scars that may be improved by resurfacing techniques may be treated early (6–8 weeks) in the wound healing process where the redness from the early inflammation is blended with that of the resurfacing process. Cheek scars that cause retraction or distortion of the lower eyelid, nostril, or lip are likely to worsen with scar maturation and can be revised early.
Cheek scar revision techniques
Several surgical and nonsurgical techniques are available for improving the appearance of cheek scars. The technique selected depends on the attribute of the scar that needs to be improved. Compared with other facial subunits, the cheek has ample skin and most scars in this region can be revised using surrounding tissue.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


