Trapezoidal Paddle Pectoralis Major Myocutaneous Flap for Esophageal Replacement
B. STRAUCH
C. SILVER
R. FEINGOLD
A. SHEKTMAN
EDITORIAL COMMENT
The pectoralis major myocutaneous flap for intraoral reconstruction has a high failure rate caused mainly by inadequate positioning of the skin paddle. The trapezoidal design of the skin paddle, which is placed entirely over the pectoralis major muscle, gives assurance of excellent viability and decreases the complications of intraoral skin necrosis. This alternative is useful in free-flap resurfacing intraorally.
The trapezoidal paddle pectoralis major myocutaneous flap is especially useful for circumferential hypopharyngeal defects and for esophageal reconstruction in elderly patients. It is preferred by the authors to free jejunal autografts.
INDICATIONS
Reconstruction of circumferential defects of the hypopharynx and cervical esophagus remains a challenge. Correction can be accomplished with the use of pedicled myocutaneous flaps or with the use of microvascular free flaps. The trapezoidal paddle pectoralis major myocutaneous flap (TPPMMC) is recommended and preferred for its ease of performance over free jejunal flaps, for the rapidity of surgery, and for the absence of an intraperitoneal approach.
Generally, malignant disease in this area carries a poor prognosis; therefore, surgical intervention frequently assumes only a palliative role. For this purpose, a procedure needs to have a low rate of major complications and also should allow the patient to return to a normal or near-normal lifestyle as soon as possible after surgery. Reconstructive efforts should be easily executed, should require little in the way of expensive equipment, and should conserve hospital resources. The trapezoidal paddle pectoralis major myocutaneous flap represents such a procedure.
ANATOMY
The pectoralis major is a type-V muscle, with its dominant vascular supply coming from the pectoral branch of the thoracoacromial artery running on its undersurface. The skin island and muscle are raised together using the origin of the thoracoacromial vessels at the clavicle as the axis of rotation. All the skin attached to the muscle will survive elevation as a myocutaneous flap.
FLAP DESIGN AND DIMENSIONS
The skin island is drawn on the chest wall as a trapezoid, with the shorter parallel side superiorly and the longer parallel side inferiorly. It is situated entirely over muscle with no “random” portion. The height of the trapezoid corresponds to the length of the pharyngoesophageal defect. Once tubed and transposed, the superior narrow base of the trapezoid will become situated in the inferior pole of the defect to be anastomosed to the esophagus. Therefore, the width of this component of the trapezoid must correspond to the diameter of the esophagus. Because this distal suture line represents the narrowest portion of the reconstruction, an 8-cm width is usually required to prevent stricture. After transposition, the inferior wider base of the trapezoid will become situated in the superior pole of the defect, to be anastomosed to the oropharynx. Thus, the width of this component of the trapezoid must correspond to the diameter of the oropharynx.
OPERATIVE TECHNIQUE
After the extirpative part of the procedure is completed, the resultant defect is measured. The vertical height of the defect will become the vertical height of the trapezoidal paddle. The skin paddle is outlined on the chest wall in a trapezoidal shape, with the long edge of the paddle placed inferiorly and the short edge placed superiorly (Fig. 219.1). The length of these edges should be equal to the circumference of the oropharyngeal and esophageal remnants. The skin paddle should lie entirely over the pectoralis major muscle. No “random” portion should be created.
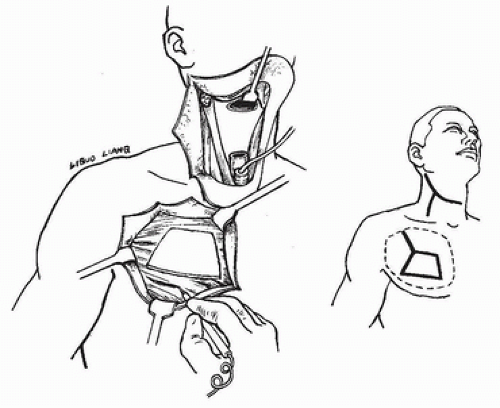 FIGURE 219.1 After extirpation, resultant defect is measured. Vertical defect height will become vertical height of the trapezoidal paddle. Skin paddle is outlined on chest wall in trapezoidal shape, with the long edge of the paddle placed inferiorly, and the short edge is placed superiorly.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





