Chapter 36 TransFix Anterior Cruciate Ligament Femoral Fixation
Background
More than 100,000 anterior cruciate ligament (ACL) reconstructions are estimated to be performed annually in the United States.1,2 There has been a tremendous amount of research on both graft selection and fixation methods.3–5 The increased use of soft tissue grafts and the concern regarding soft tissue interference screw fixation (e.g., graft pullout, slippage, damage) have led to the development and use of femoral cross-pin fixation in ACL reconstruction. One successful technique for cross-pin fixation is the TransFix ACL reconstruction technique (Arthrex, Naples, FL).
Biomechanical and Clinical Results
The Arthrex TransFix implant is made of titanium, and the Bio-TransFix implant is made of poly-L-lactic acid (PLLA), as shown in Fig. 36-1. In vivo, the Bio-TransFix implant hydrolyzes into lactic acid, which is then metabolized into CO2 and H2O. A proprietary degradation study of the Bio-TransFix demonstrated that it does not lose shear strength through 52 weeks.

Fabbriciani et al used the TransFix system in conjunction with fresh, ovine, doubled Achilles tendons and ovine femurs.5 Cyclical loading comparisons of bioabsorbable and metal RCI screws (Smith & Nephew, Andover, MA), the LINX HT (Mitek, Norwood, MA), and the TransFix implant showed significantly lower mean values of graft elongation for the TransFix construct (1.5 ± 0.1 mm) over 1000 cycles. The maximum load to failure (LTF) for the TransFix was 890N ± 175N, which, unlike the other devices in the study, is comparable to that of the intact ovine ACL (725N ± 77N).
Becker et al showed that the stiffness of the TransFix construct (184 N/mm) approximates the stiffness of the human ACL (242 N/mm, as reported by Woo et al6) and provides significantly greater ultimate strength than interference screw fixation.7 This study compared three fixation methods using a porcine femur model: (1) TransFix fixation of a quadruple tendon, (2) 8- × 20-mm biodegradable interference screw fixation of a quadruple tendon, and (3) 8- × 20- mm titanium screw fixation of a patellar tendon–bone graft using a porcine femur model. Interference screw fixation of the patellar tendon and quadruple tendon resisted only 59% and 37%, respectively, of the pullout strength of the TransFix (1303N ± 282N). The TransFix had significantly less construct displacement during cyclical loading than the interference screw/quadruple graft construct.
Ahmad et al demonstrated that interference screw fixation and the Rigidfix cross-pin technique were inferior to the Bio-TransFix and the Endobutton for graft slippage during cyclical loading and ultimate LTF.8 After 1000 cycles, the graft displacement for the Bio-TransFix was 1.13 mm compared with greater than 5 mm for the interference screw and Rigidfix. This study also showed significantly greater LTF of the Bio-TransFix (746N ± 119N) as compared with the interference screw technique (539N ± 114N).
As these and other studies have demonstrated, the use of the TransFix system offers considerable advantages compared with other femoral fixation systems in terms of yield load, stiffness, and deformation and elongation under cyclical loading. These results offer stable fixation of the graft during the postoperative period, before graft healing has occurred. The inherent rigidity of the TransFix limits graft-tunnel motion during physiological loading. Intratunnel motion has been associated with tunnel widening.9 Fauno and Kaalund reported a significant reduction in tunnel widening in the femur when TransFix was used compared with Endobutton fixation at 1-year follow-up for a prospective randomized study.10 Unlike interference screw techniques, in which the graft is squeezed and possibly damaged during screw insertion, graft strength is maximized with the TransFix technique.
In 1998, Wolf11 reported his initial results with the TransFix fixation. Eighty-eight percent of patients at follow-up described their postoperative knees to be normal or near normal. The 27 patients had a mean KT-1000 side-to-side laxity difference of 1.5 mm at follow-up. (Ahmad reports that greater than 5 mm may be considered clinical failure.8)
Recently, Harilainen et al12 showed no significant difference in IKDC scores at 2-year follow-up for TransFix cross-pin fixation versus metal screw fixation. In this controlled prospective randomized study, 85% of the TransFix group and 73% of the screw patients were in the IKDC A or B categories.
Surgical Technique
The TransFix technique requires that a 3-mm drill pin be passed from lateral to medial. Although no neurovascular complications have been reported, theoretically the medial (and lateral) neurovascular structures are at risk. The author’s lab has shown that a defined “safe zone” exists in which a distal femoral cross-pin can be reliably placed without damaging the local neurovascular structures.13 In this anatomical cadaveric study, the absolute neurovascular safe zone during cross-pin guidewire placement is from +20 degrees (0 degrees equals “parallel to the floor” line) and –40 degrees (lowering the guide more posteriorly) (Fig. 36-2).
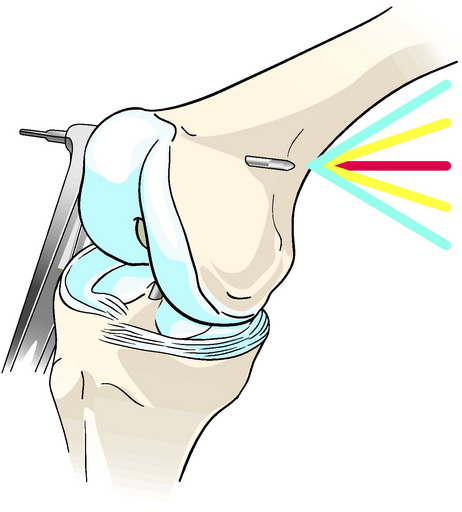
Fig. 36-2
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


