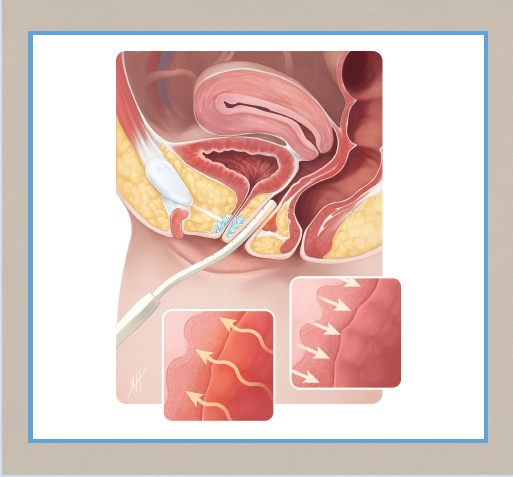
CHAPTER 16 • Temperature-controlled radiofrequency (RF) tightens vulvovaginal tissues immediately and over a period of several months and is effective for nonsurgical vulvar and vaginal tightening. • Temperature-controlled RF encourages new collagen formation and neoangiogenesis, resulting in improved skin tone and sensitivity. • Tightening of vaginal tissues reduces vaginal laxity, stress incontinence, overactive bladder, and mild to moderate cystocele and rectocele. • Temperature-controlled RF results in improved vulvovaginal blood flow that normalizes vaginal moisture and improves overall sensitivity of the clitoral, vulvar, and vaginal tissues. • Orgasmic dysfunction may be aided by temperature-controlled RF treatments. __________ I first used radiofrequency for precision labial surgery in 2005. The concept for intravaginal and vulvar use of radiofrequency became a reality in 2009-2010 when I performed the first radiofrequency treatments on the vulvovaginal area for aesthetic benefits of tissue shrinkage. In 2013 I started development of ThermiVa (Thermi), a specific device intended for use on both the vulva and the deep vagina for the purpose of dermal skin tightening and vaginal tightening. Clinical research showed that the vaginal and anal mucosal treatments and tissue tightening also aided in relief of stress incontinence, overactive bladder, mild to moderate cystocele and rectocele, orgasmic dysfunction, and fecal incontinence. I continue to consult with Thermi and perform clinical studies on the effects of temperature-controlled RF in vulvovaginal tissues. ThermiVa is FDA approved for dermatologic conditions and surgical nerve ablation in the United States. Examples of dermatologic conditions are loose skin, dry skin, and insensitive skin. ThermiVa does not currently have specific FDA approval for vaginal or anal tightening, vulvovaginal atrophy, stress incontinence, overactive bladder, pelvic prolapse, fecal incontinence, and organic dysfunction. I receive royalties from the sale of ThermiVa generators and wands. Between childbirth—often multiple childbirths—and waning estrogen levels from menopause, the vagina undergoes numerous changes that lead to a well-defined suite of conditions that begins with vulvovaginal laxity with reduced elasticity and includes atrophic vaginitis (leading to chronic irritation and discomfort), stress urinary incontinence, and different manifestations of sexual dysfunction. Any or all of these may be present, and the age of onset may vary. Addressing these conditions is problematic because of two factors. First, women have traditionally had difficulty discussing these issues with their primary care physician or gynecologist. Until recently, social mores were responsible for a dim view of frank discussions about the vagina, and the societal attitude toward these conditions was one of resignation. Second, physicians’ armamentarium has been anything but comprehensive, limited to hormone therapy, Kegel exercises to strengthen the pelvic floor, the use of creams or lubricants, and more invasive surgical options. Energy-based modalities have been applied to this tissue in the same fashion as in aesthetic medicine, with the purpose of causing collagen denaturation and contracture, stimulating neocollagenesis and feminine restoration through the healing cascade from the heating of tissue. This thermal effect induces the production of fibroblasts and stimulates neocollagenesis. Intuitively, the ability to deliver more energy will cause a more profound effect, to a point. Directed energy does not cause the sensation of pain in the vaginal wall as readily as it does in facial skin, making energy-based therapies more tolerable at higher energies, and suggesting that the vagina may be an ideal anatomic region for energy-based resurfacing of tissue. Regardless of which term is used—rejuvenation, resurfacing, tightening, or treatment of laxity—the basic aims and methods are similar. Tissue contraction using RF energy is an established modality in aesthetic medicine.1,2 Heat is generated in proximity to the electrode through impedance as RF energy travels through tissue, which can be calculated using an equation accounting for local electrical conductivity and the level of current generated near the electrode (RF emitter).3 This specific pattern of thermogenesis is thus predictable and can be controlled by modulating power to the electrode itself. Therapeutically relevant heating of tissue has been shown to lie within a recognized temperature range (40° to 45° C) to optimally stimulate neocollagenesis and neoelastinogenesis while minimizing collateral damage to skin and nearby tissue structures; RF energy must therefore be controlled in relation to tissue temperature during therapy to maximize energy delivery, yet prevent overtreatment. Unlike other proven energy-based methods, RF is completely noninvasive; thus skin barrier function is preserved, minimizing healing time and patient risk. Because RF does not use light energy, skin pigmentation is not a factor in treatment. RF energy is especially suited for naturally moist and well-hydrated tissue such as that of the vaginal wall and vulva.4 Transcutaneous temperature-controlled RF (TTCRF) therapy, brand name ThermiVa, employs a monopolar RF electrode and return pad (to complete the circuit), between which electric current is passed.3,4 Power to the RF emitter is automatically modulated by thermistors and thermocouples integrated into the treatment device to monitor local tissue temperature in real time. Thus temperature targets may be safely achieved rapidly and maintained for a duration sufficient for therapeutic tissue response. Proper management of tissue temperature has a positive impact on patient comfort during treatment; treatment is very comfortable and no anesthesia is necessary. For vaginal applications,4 TTCRF technology is contained within a treatment probe approximately 20 cm long and 1.5 cm wide (about the width of an adult finger) with a shallow S curve toward the center, similar to that of a Hegar dilator (Fig. 16-1). The slim treatment probe has the advantage of reducing potential trauma from insertion resulting from dryness, sensitivity, and atrophy of vaginal wall tissue. The RF emitter (about the size of a postage stamp) is located on one side of the probe tip.
Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
Red Alinsod
Key Points
Related posts:
 Fractional Erbium Laser for Vaginal Rejuvenation
Fractional Erbium Laser for Vaginal Rejuvenation
 Augmentation of the Labia Majora With Fillers
Augmentation of the Labia Majora With Fillers
 Informed Consent and Liability in Cosmetic Genital Surgery
Informed Consent and Liability in Cosmetic Genital Surgery
 O-Shot®
O-Shot®
 Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
Transcutaneous Temperature-Controlled Radiofrequency for Vulvovaginal Rejuvenation
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine
