CHAPTER 7 TRAM Flap Variations in Breast Reconstruction
Summary/Key Points
Patient Selection
Patient selection as in other surgical procedures is of critical importance in the success of breast reconstruction and in particular in the area of autologous breast reconstruction. Carl R. Hartrampf who developed and popularized the TRAM flap (originally termed by him as the transverse abdominal island flap) developed a strict criteria for patient selection that included patient risk factors as well as surgeon experience.2
Once it has been determined that the patient is a candidate for breast reconstruction and has the desire and realistic expectations of what this involves, a more thorough evaluation of the patient can proceed for surgical repair.3,4 The risk factors that keep coming up in studies as most significant include obesity, a strong smoking history, significant metabolic or cardiovascular compromise and a history or intention of using radiation therapy to the breast cancer site. These risk factors need to be considered individually and in combination in order to make a final decision whether breast reconstruction should be performed and what type is most appropriate. This chapter will concentrate on variations of the traditional TRAM flap that can in certain situations improve the chance of a successful outcome.
Indications
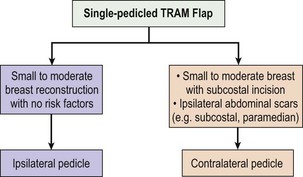
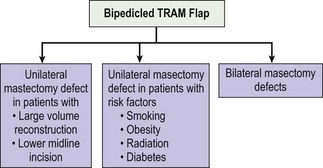
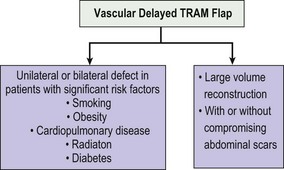
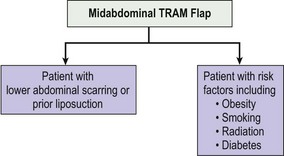
TRAM flap reconstruction can give a very satisfying outcome to the patient who has recently experienced the shock and hardship of a diagnosis of breast cancer. It does however require a considerable investment of time and effort on the part of the patient and the surgeon in order to achieve optimal results. The TRAM flap can also be used for other forms of chest reconstruction resulting from tumor excision or congenital problems such as Poland’s syndrome. It has been used very effectively based on the more robust inferior epigastric pedicle for pelvic and perineal reconstruction due to tumors, trauma, and other causes requiring a large volume of well vascularized tissue. The algorithmic flow charts in Figures 7.1, 7.2, 7.3 and 7.4 show the indications for the TRAM flap and its variations based on morphologic and treatment characteristics.
The most common indication for TRAM flap reconstruction is for a patient with breast cancer who will undergo or has undergone some form of mastectomy. This brings up the issues of immediate or delayed reconstruction which has again become a timely concern with the increasing use of adjuvant radiation therapy for breast cancer. Many studies over the years have shown that immediate reconstruction is a very good option.5 It does not add to the oncologic risks to the patient whether a traditional mastectomy or the increasingly popular skin-sparing mastectomy is performed.6,7 It also permits the surgeon to perform an excellent reconstruction knowing how much breast tissue and volume have been removed, working with native tissues unaffected by scar and contracture, and having a three-dimensional image of the needs for reconstruction. It also permits the patient to recover more quickly overall from the ablative and reconstructive procedures. A psychological benefit in not experiencing a loss of the breast has also been noted, although there are recent counter-arguments in this regard.7 However if post-mastectomy radiation therapy is indicated this will adversely affect the aesthetic outcome of the reconstructive procedure. This has been shown in cases of immediate and even delayed reconstruction.8 The major problem arises when the decision for radiation therapy is determined after the operation when the final pathology of the specimen is determined. This usually occurs about one week after the mastectomy procedure. Several centers will prescribe delayed reconstruction in the patients with a high risk or a high potential for post-mastectomy radiation therapy. At times, reconstruction is temporized by placing a tissue expander in the mastectomy pocket that will be removed after radiation therapy or at the time of the delayed TRAM flap reconstruction.9
Other contraindications for TRAM flap reconstruction are significant systemic disease such as cardiovascular and respiratory problems as well as insulin-dependent diabetes. Hartrampf included insulin-dependent diabetes as one of his significant risk factors. Other groups have not placed as much importance with this.10 I personally have experienced some significant infectious complications in patients with insulin-dependent diabetes and so I am particularly cautious in these patients.
Morbid obesity and smoking have been shown in several studies to be significant risk factors in all forms of breast reconstructions including the TRAM flap.11,12 Variations of the TRAM flap need to be considered in these cases. In the morbidly obese, a midabdominal TRAM flap, a delayed or a double-pedicled TRAM flap may be indicated if it is decided to do any surgery at all. Similarly, in a chronic smoker or one that has recently quit, these TRAM flap variations may also be useful. All attempts, of course, should be made for weight reduction and cessation of smoking prior to performing autologous breast reconstruction.
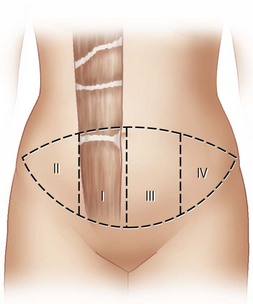
The experience and comfort level of the surgeon and the surgical team is an important factor in the final indication and decision for a particular type of breast reconstruction. The relative ease and decreased time of performing a TRAM flap makes it a most desirable method of reconstruction. However the surgeon should discuss the various options available in an honest and humble manner with the patient prior to making the final decision. Our understanding of the vascular supply of the TRAM flap is based on a great number of anatomical studies. The more recent classification of Ninkovic et al has refined our understanding of the zones of perfusion. This classification places more importance on the ipsilateral perfusion than the older Hartrampf classification that assigned greater importance across the midline (see Fig. 7.5).
Operative Technique
Preoperative preparation
The preoperative preparation of the patient should be well structured and thorough. The amount of time and effort that goes into this preparation will reap benefits intraoperatively as well as in the postoperative period. Any imaging or non-invasive vascular studies, such as laser Doppler flow studies, or computerized tomography (CT) angiogram13 can be conducted preoperatively in order to get a good assessment of the vasculature of the lower abdomen and chest. This is not a substitute for careful operative dissection but can be useful in patients with risk factors that may also include previous scars on the abdomen. Preoperative marking is very important and should be done with the patient in a standing position. Scars of the abdomen are noted; they may include an upper or lower midline scar, appendectomy scar, paramedian scar, or a Pfannenstiel incision. All of these will impact on the type of TRAM flap that will be proposed as well as the incision of the flap. For instance, a lower midline incision may dictate a double-pedicled TRAM flap if a large volume of tissue is needed for reconstruction. The size of the contralateral breast is also taken into consideration. If any modifications are going to be made during the procedure or in a subsequent operation, this also needs to be taken into account. If it is an immediate reconstruction, the size and weight of the mastectomy specimen will be readily available. If it is a delayed reconstruction, it is useful to ascertain the size and weight of the prior mastectomy specimen. This was a very important piece of information to Hartrampf in deciding and predicting the amount of tissue needed for reconstruction. The midline of the abdomen from the xiphoid to the pubis is drawn. A lenticular or transverse elliptical pattern is then drawn on the lower abdomen. An attempt to establish symmetry on both sides is made. The anterior–superior iliac spines are delineated and used in the markings. A pinching of the lower abdominal tissue in order to get an idea for closure is then performed. Adjustments are made according to the ability to be able to close the abdominal wound once the flap has been raised.
The patient is placed in a supine position and general endotracheal anesthesia is induced. A Foley catheter is placed and checked to be in good working condition. Sequential compression devices are now applied to both lower extremities. If the patient is at high risk for DVT or pulmonary embolus, prophylaxis with low molecular weight heparin or other indicated prophylactic drugs are given. Guidelines that include a list of risk factors should be followed to help in preventing thromboembolic disease.14 Blood is screened but not cross-matched for possible transfusion which has become rare in ablative and reconstructive breast procedures.
Surgical technique
Variation I: double-pedicled TRAM flap
The operative technique for a single-pedicled and double-pedicled TRAM flap (DPTF)15 reconstruction initially is similar. Since the DPTF is much better vascularized, a larger flap can be drawn on the abdomen as both rectus muscle pedicles will be used (see Fig. 7.6
Related posts:
 Saline Implants: Getting a Good Result
Saline Implants: Getting a Good Result
 Surgery of the Breast in Poland’s Syndrome
Surgery of the Breast in Poland’s Syndrome
 Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
 Autologous Flap Use in Breast Reshaping after Massive Weight Loss
Autologous Flap Use in Breast Reshaping after Massive Weight Loss
 Fat Injections to the Breast: The Lipomodeling Technique
Fat Injections to the Breast: The Lipomodeling Technique
 Subfascial Breast Augmentation
Subfascial Breast Augmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


