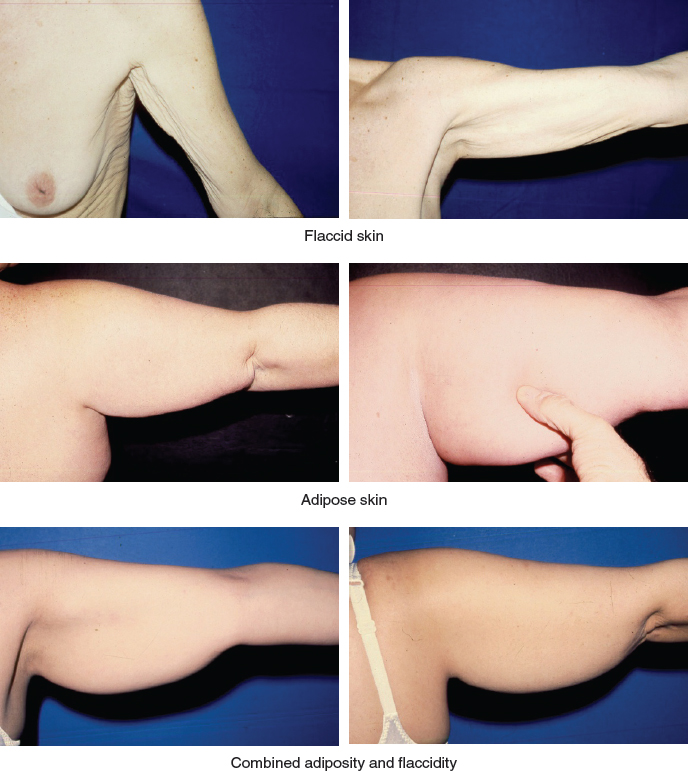
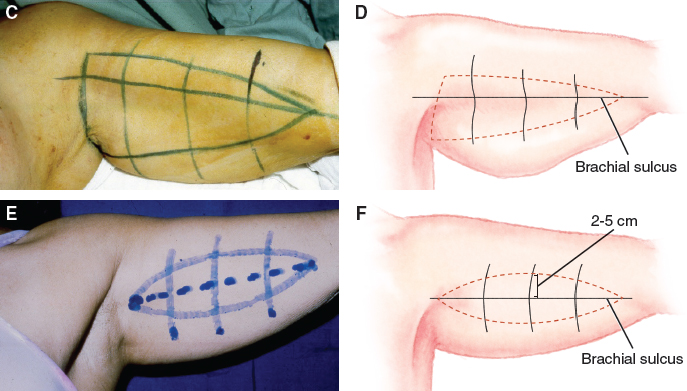
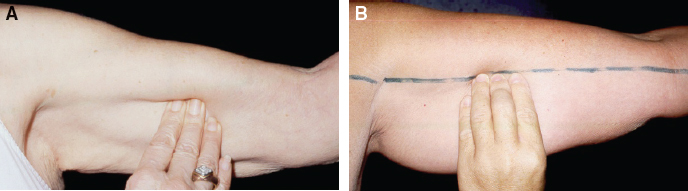
CHAPTER 10 As with any type of plastic surgery, if the patient exhibits an excess of vanity in the presence of dysmorphic disorder, the surgery is contraindicated. Regardless of the type of surgery being considered, the costs and benefits should be evaluated. These include an accurate assessment of everything that will be involved in the process as well as a consideration of the scar that will be left when the procedure is complete. For patients with skin dystrophy of the upper arms, surgery has become a routine solution. This surgical request is more common among individuals who live in tropical areas, where brachioplasty is requested more frequently as a result of the increased level of arm exposure. The literature that discusses brachioplasty dates to 1945, and contributions and refinements continue to be made. With the introduction of bariatric surgery into the surgical armamentarium, the significant weight loss associated with it has created a new group of formerly morbidly obese patients with a different set of dysmorphophobic beliefs. These patients have a large volume of adipose tissue that is irregularly distributed throughout the body, and there has been a change in the quality of their elastic fibers. These two factors bring many surgical inconveniences as well as the aesthetic and psychological concerns that are quite familiar to plastic surgeons. Information should be provided to these patients preoperatively through photographs of other patients’ brachioplasties, as well as all of the details about the specific problems that were addressed for previous patients. There are three basic types of skin problems of the upper arm for which patients request solutions: excessive skin flaccidity without adiposity, localized adiposity from the shoulder to the elbow without skin flaccidity, and combined adiposity and flaccidity. Brachioplasty is restricted to the anterior, posterior, medial, and lateral aspects of the upper arm. It is limited to the area between the axilla and the elbow in almost all cases. The rare cases in which flaccidity extends to the forearm can be addressed with specific surgical procedures that are beyond the scope of this chapter. The surgery is restricted to the skin that is connected to the fascia, which holds the muscles like a glove. The extension of these tissues should be preserved to avoid severing the muscles, nerves, and vessels. The fascia continues to the axilla and covers the deltoid, the pectoralis major, the infraspinatus, and the forearm muscles without interruption. Along the brachial axis, the fascia has an internal and an external septum that divide the upper-arm cylinder into two muscular segments: the flexor anterior group and the posterior area with the extensor muscles. These are visible in the skin, and they are called the internal and external brachial sulci. The nerves and vessels contained in the subcutaneous tissue are of limited importance if they will be resected during surgery. Two veins run in the upper arm: the cephalic vein, which runs along the external brachial surface; and the basilic vein, which is found near the internal brachial sulcus and which crosses the fascia at its midsegment. The lymphatics end at the axilla in a netlike formation. Anatomic Danger Zones ■ Near the elbow there is a superficial lymphatic plexus that, if severed during surgery, produces edema that may persist for several weeks. A more dramatic situation may occur if the axillary lymph nodes are removed. ■ The sensory nerve that supplies the skin of the external surface of the arm is the circumflex nerve. The internal brachial nerve and its accessory nerves supply the internal aspect of the arm. These superficial vessels and nerves are important and must be preserved during surgery. Injury of the basilic vein may cause prolonged edema with pain and eventually result in long-term local fibrotic reactions. The previously described surgery has a high physiologic and aesthetic level of patient satisfaction, when executed within the described procedures. The safe limits are narrow and the attention must be continuous. Prudence and care have to be used in all of the surgical aspects and during the first postoperative month. Special written recommendations are offered to the patients for control with the routine during the first postoperative year. Patients who are candidates for this type of surgery are unsatisfied with their arms. They do not like to expose their arms, they usually wear clothes with long sleeves, and the desire to have surgery only becomes part of their plans when other noninvasive methods fail. Based on the safety aspects of the surgical procedures, complications rarely occur. When such problems occur, the responsibility is usually with the doctor who has performed the procedures and rarely with the patients who did not remain within the limits allowed. Indications and contraindications for surgery are related to the type, volume, and shape of the upper arms, which is generally out of the proper aesthetic limits of this region. As in all other regions of the body, psychological behavior should be taken into account, to avoid unnecessary surgery. It is fundamental to orient patients about all steps of the surgery, combined with illustrative photographs about the position of the scars, the quality of the results, and also all limitations and possibilities. This includes surgery revision, which is directly related to the extension of the operation. It is imperative to show photographs of preoperative and postoperative photographs of similar cases, and to offer pamphlets about all the details related to the surgery, including the limits and possibilities, postoperative care, scar revision, keloids, hypertrophic scars, and so on. Like any other type of aesthetic plastic surgery, the patient-doctor relationship should be integrated from the first consultation up to the end of the treatment when the last question is asked about whether the patient is happy with the result. In our viewpoint, it is the doctor’s responsibility to offer surgery revision up to 1 year after the surgery, according to previous information. In general, the candidates for this type of surgery already have knowledge about the quality of the results, the type and place where the scar should be positioned, and so on. In addition, patients should also be informed about scar revision as part of their treatment. Information and photographs of previous brachioplasty patients should be part of the first consultation, particularly for patients who do not have any preexisting scars on their body. The evaluation of the deformity should include determining whether the patient has excessive skin flaccidity without adiposity, localized adiposity without skin flaccidity, or combined adiposity and flaccidity. As previously described, depending on the deformity, a different approach will be used. Isolated brachioplasty can be done in an ambulatory or a day-clinic environment. The amount of skin to be removed is evaluated by a pinch test and, whenever necessary, the areas of excessive fat are also marked. Sedation and local infiltration are sufficient for most patients. When combined with other procedures, the management of the patient must change according to the extent of the operation. Fig. 10-2, A and B Surgical markings are made with the patient in the standing position with the arm abducted at 90 degrees. The markings start at the internal brachial sulcus and move from the axilla to the elbow. The palpation and demarcation of the internal brachial sulcus are shown in Fig. 10-2. It is easier to identify the internal brachial sulcus in slim patients by palpation. Skin markings are also easier in thinner arms, because the excess skin to be removed is clearly estimated compared to more adipose arms. The amount of skin to be resected is estimated with a pinch test that involves the creation of an elliptical shape drawn a few centimeters above the internal brachial sulcus, which is used as a reference point. The broadness and extension of the ellipse change with the amount of skin to be resected. In general, the ellipse’s superior line is positioned 2 to 5 cm above the internal brachial sulcus. Parallel vertical lines are drawn perpendicularly to the demarcation of the ellipse to serve as a guide and to facilitate the closure. The skin resection varies according to the local forces and skin excess. The axillary skin excess resection is specific for each case. Depending on the excess skin in this particular area, the resection of excess axillary skin may end on a straight resection at the end of the fusiform excision or on a T or V scar. This parallel and transverse line is designed along the helicoid or triangular skin demarcation, serving as a type of guide to adjust the suture line. The resection of the excess skin is not performed according to a specific procedure. It varies according to the local excesses. The surgeons who are dedicated to performing upper arm surgery must be familiar with this detail. The resection of excess axillary skin is specific for each case. In general, it may have a T or V scar, a straight resection, and so on. They are placed according to the skin excesses to be resected, and it is important that the dissection must be superficial to avoid severing the structures underneath.
Traditional Approach to Brachioplasty
Surgical Anatomy
Physiologic Considerations
Indications and Contraindications
Patient Evaluation
CLINICAL EVALUATION OF THE DEFORMITY
Preoperative Planning and Preparation
Surgical Technique
ANESTHESIA
MARKINGS
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine