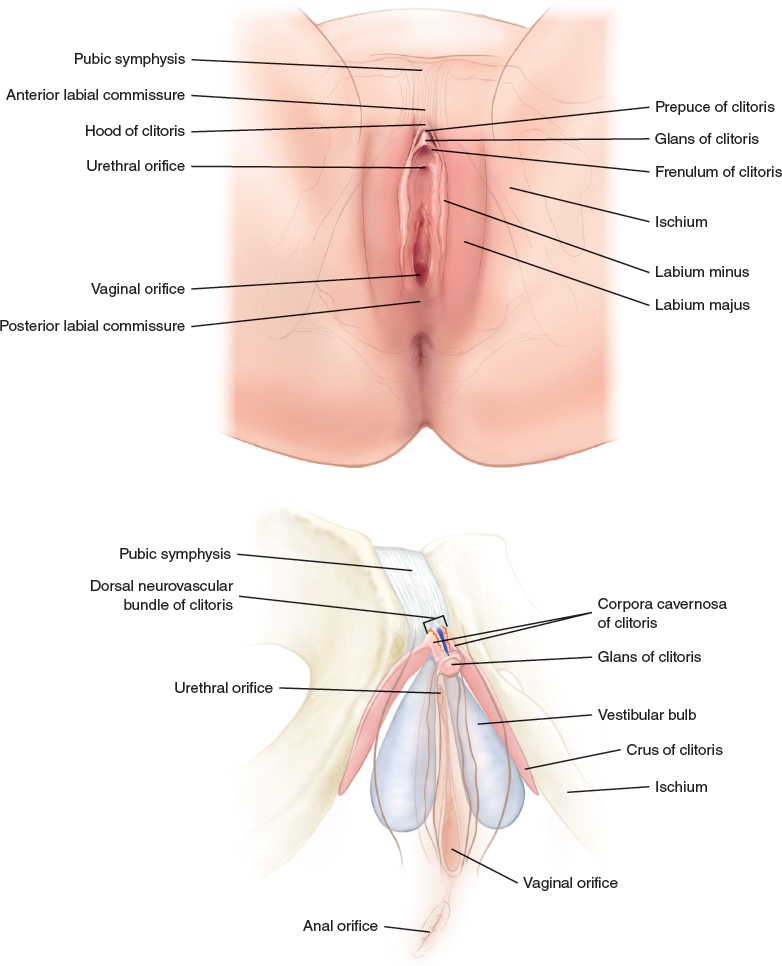
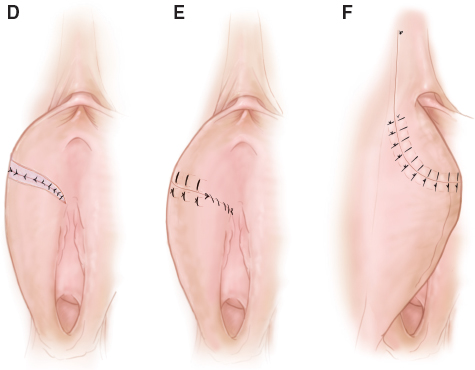
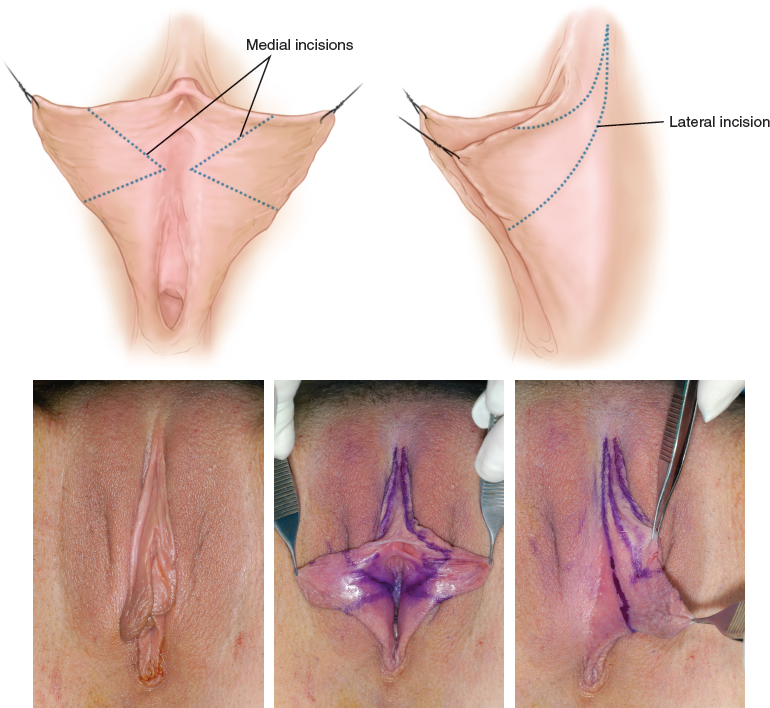
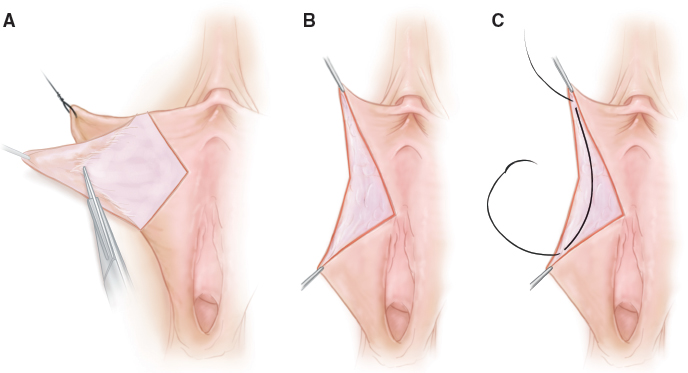
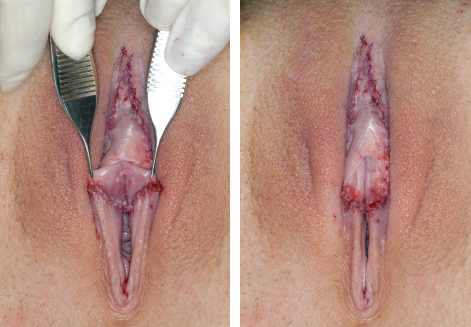
CHAPTER 22 In general, most people consider female aesthetic ideals as (1) symmetrical labia minora (inner lips) that do not overhang past the labia majora (outer lips) on standing, (2) a relatively short clitoral hood with few ridges that is not overly projecting, (3) full, but not bulging, labia majora with no excess skin, and (4) a mons pubis fat pad that does not protrude when the patient is wearing clothes. Fortunately, successful procedures have been developed which are able to achieve most patient goals. Most women with enlarged labia minora, majora, and/or the clitoral hood also complain of some discomfort with clothes, exercise, or intercourse. Anatomic Danger Zones ■ Urethral orifice ■ Dorsal neurovascular bundle of the clitoris ■ Corpus cavernosa of the clitoris ■ Glans of the clitoris ■ Crus of clitoris Knowledge of clitoral anatomy is essential to prevent an injury or negative change in sexual sensation. The anatomy of the clitoris is similar to that of the penis, because they are homologs. The glans (head) of the clitoris is visible under the overlying prepuce of the clitoral hood. The shaft of the clitoris is composed of two corporeal bodies that are attached to the pubis symphysis by the suspensory ligament of the clitoris. The corpora diverge and attach bilaterally to the ischium. Paired ventral ridges of skin (frenula) extend from the glans clitoris. Each labium minus is formed from the convergence of the frenulum of the glans clitoris with the lateral clitoral hood. A labium may gradually taper down and be minimally present posteriorly or extend and meet the opposite labium at the posterior introitus. The body of the clitoris is easily palpated. Pubic fat excision can be safe if resection is performed superior to the pubic symphysis. Labia majora fat excision will not injure the clitoris if the resection is superficial to the ischium and lateral to the pubic symphysis. Labia minora enlargement is usually congenital but becomes more obvious in adolescence. Pregnancy, birth control pills, aging, hormonal disorders, and exogenous hormones can also increase labial size. The ideal labia minora are thin, light-colored, straight, nonredundant, and symmetrical. Traditionally, and most commonly, labia minora reduction is performed by trimming the labial edges using a scissors, scalpel, clamp, or more recently, a laser. The long labial edge suture line often results in a scalloped, wide, irregular labial edge, even if closure is performed with interrupted, running, or subcuticular sutures. Overresection with partial or complete labial removal can occur. Because the leading labial edge is a suture line, there is a higher incidence of chronic discomfort. In addition to the difficulty attaining smooth, symmetrical labial edges, it is very troublesome to achieve a natural transition from the labial edges to the clitoral hood and clitoral frenula. Releasing the frenula may also cause the clitoral hood to move anteriorly, making it more protuberant, with a larger appearance. The advantages of the trimming technique are the lighter resulting color of the labial edge and the shorter operating time, and it is still the most common labia reduction procedure. However, because the trimming techniques can lead to many patient complaints, the extended central wedge procedure was developed, which includes partial clitoral hood reduction. A woman is a candidate for labia minora reduction if she considers her labia minora to be too large or protuberant. Because labia minora vary dramatically between women, reductions can be small to large. There may also be minor or dramatic asymmetry of the labia or clitoral hood that can usually be corrected during surgery. Caution must be exercised when operating on women with vulvar pain syndromes, because these may be exacerbated with surgery. The patient should be evaluated in the lithotomy position, with the woman viewing her vulva with a hand mirror. The labia are examined for the amount of protrusion, width, color, symmetry, and anterior and posterior length. The clitoral hood should be assessed for thickness, protrusion, redundant folds, the location of hyperkeratotic skin, glans size, and glans exposure. The posterior introitus should be examined for a high posterior lip or an open introitus, which is usually associated with an episiotomy. Vaginal laxity and a short perineum are evaluated. A pigmented perineal raphe or hyperkeratotic perineal tissue may be present that the patient may wish to have excised. The central wedge excision usually includes the most protuberant and most darkly pigmented portion of the labium. The wedge is adjusted in size to achieve symmetry. The patient is shown the projected postoperative appearance by holding the anterior and posterior portion of the V excision together in each hand while the patient is lying down, watching with the mirror. Occasionally, there is a color mismatch between the anterior and posterior labium at the anastomosis, but this is rarely an issue if it is shown to the patient preoperatively, and it usually is less noticeable with time. The area of the clitoral hood that will be excised is also shown. If a high posterior lip needs to be revised or a perineoplasty is to be performed, this must be explained to her. A very large, wide labium may require two wedge excisions on each side or a wedge excision with a lateral, and possibly also a medial, elliptical posterior excision. The patient must be told and shown the exact plan and the projected result to prevent any misconceptions or false expectations. An informed consent is obtained, and educational materials and media may be offered. A routine labiaplasty can be performed with the patient under general anesthesia, sedation, or local anesthesia. Because the procedure is performed with the patient in lithotomy position and takes an average of 1½ to 2 hours, the patient may become restless under local anesthesia. Fig. 22-2 The markings are made to excise the most protuberant area of each labium with a wedge or V excision. The upper marking is usually made at the junction of the frenulum with the clitoral hood to form the labium or just posterior to this convergence. The procedure is performed with the patient in the lithotomy position with armboards. The patient is prepped and draped, and the surgical area is infiltrated with lidocaine with epinephrine and bupivacaine (Marcaine). Loupe magnification is very helpful in achieving excellent closure. Fig. 22-3, A-C The mucosa of the medial labium is removed, leaving as much subcutaneous tissue as possible. Lateral skin is then removed with no subcutaneous tissue being removed. The subcutaneous tissue is reapproximated using 5-0 Monocryl on a TF atraumatic needle. A two-layer closure of good subcutaneous tissue helps prevent wound dehiscence or perforations. Medial or lateral excess subcutaneous tissue is excised during closure to prevent dog-ears or excessively thick labia. Fig. 22-4 The external closure starts at the distal leading tip with sutures of vertical mattress 5-0 Monocryl sutures on a TF needle. Vertical mattress sutures are used on much of the lateral and medial closure. Running 5-0 Monocryl sutures are used deep medially and often laterally. Excess skin and mucosa are trimmed during closure. The lateral clitoral hood excision is closed with a running 5-0 Monocryl suture in the subcutaneous tissue and a running 5-0 Monocryl subcuticular closure. After completion of one side, the other is checked again for symmetry before the closure is repeated. Symmetry should be excellent at the conclusion of surgery. If a second wedge or posterior ellipses are required on one or both sides, these are performed after the bilateral anterior wedges are completed. Fig. 22-5 The lateral labial hockey-stick V extension will decrease lateral clitoral hood folds or skin excess. However, medial folds or hypertrophic skin are common, so modifications must be made. The lateral excision can be adjusted more medial in some cases. In other cases, the lateral labial V excision stops at the lateral labium and a vertical ellipse can be excised from one or both sides of the mediolateral clitoral hood. Asymmetry of the clitoral hood skin is adjusted. If the patient does not want clitoral hood excision or if no excess hood skin is present, the lateral labial excision ends at the lateral labium or lateral hood to avoid a dog-ear. If a patient has a long redundant clitoral hood or transverse clitoral hood folds, a small transverse ellipse of clitoral hood can be excised. The incision is closed with vertical mattress 6-0 Monocryl sutures. This transverse excision is rarely performed, because resection of skin can commonly cause overexposure of the glans, leading to glans hypersensitivity or an unsightly appearance. More aggressive clitoral hood reduction with clitoris repositioning (clitoropexy) is beyond the scope of this chapter. Reduction of an enlarged clitoral shaft and/or glans can also be performed, but it is also beyond the extent of this chapter.
Contouring of the Female External Genitalia
SURGICAL ANATOMY
LABIA MINORA REDUCTION
Indications and Contraindications
Patient Evaluation
Preoperative Planning and Preparation
Surgical Technique
ANESTHESIA
MARKINGS
PATIENT POSITIONING
TECHNIQUE

Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine