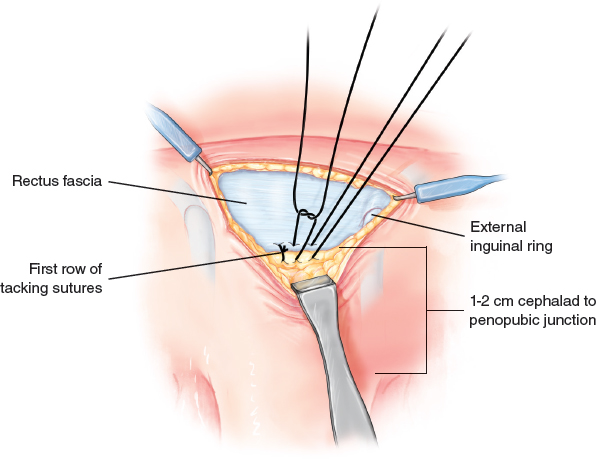
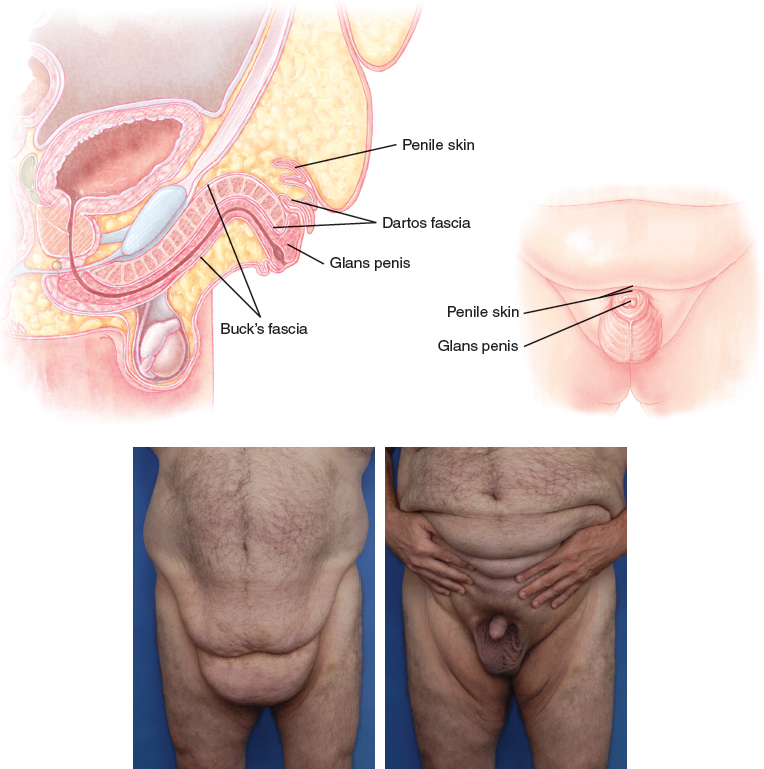
CHAPTER 23 In general, men desire a flat pubic area, a protruding penis in the flaccid state while standing or sitting, and a scrotum that preferably hangs no lower than the bottom of the flaccid penis. The patient ideally will have a straight erection without significant curvature and lacking a penoscrotal web. Most men desire as much length and girth as possible, but these enhancement procedures are controversial and investigational; therefore they are not included in this chapter. The procedures presented here successfully enhance the appearance and function of the penis, but do not enlarge it. Anatomic Danger Zones ■ Neurovascular bundles located dorsally from the 3 o’clock to 9 o’clock positions ■ The urethra The anatomy of the penis is similar to that of the clitoris; they are homologs. The glans (head) of the penis is visible under the overlying prepuce (foreskin). The shaft of the penis is composed of two corpora cavernosa erectile bodies and the corpus spongiosum (containing the urethra), which are attached to the pubic symphysis by the suspensory ligament of the penis. The corpora cavernosa diverge and attach bilaterally to the ischium. The spongiosum containing the urethra travels to the membranous urethra. The sensory nerves and blood supply are the same as in the clitoris. Fig. 23-1 A penis that is partially or completely hidden when standing, sitting, or bending is referred to as a buried, hidden, or concealed penis. Congenital buried penis is relatively uncommon but can occur in an overweight or relatively thin patient. Concealment of the penis is very common in men with aging, an overly aggressive circumcision, or excessive weight gain with or without weight loss. The underlying etiology of the buried penis is inadequate attachments of the tunica albuginea and Buck’s fascia to the dartos fascia and skin. The penile structures remain attached to the pubic bones, but the skin and dartos fascia turn inside out and telescope over the penis. A buried penis can occur in a circumcised or uncircumcised man. However, a major cause of buried penis in the circumcised man is excessive removal of the shaft skin at his initial circumcision. Inadequate penile skin prevents full penile extension. Also, removal of shaft skin instead of foreskin eliminates normal shaft skin attachments to the Buck’s fascia, which causes the penis to accordion inside. Chronic burying of the penile skin may result in the patient’s being unable to stand while voiding. The penile skin becomes chronically damp from urine and sweat, which often leads to chronic inflammation and the development of lichen sclerosus. The inflammation can cause phimosis of the distal or midshaft penile skin, with complete trapping of the glans penis. Chronic inflammation can cause destruction of the penile skin and development of penile carcinoma. Some physicians mistakenly believe that a circumcision to eliminate a phimosis will cure the buried penis, but in reality, the circumcision usually makes the situation worse. The circumcision may also remove needed skin that could be used to reconstruct the penile shaft once the phimosis is released and the buried penis is corrected. Multiple factors need to be evaluated in patients who present with a buried penis: 1. If pubic ptosis is present, the amount of skin elevation and excision needed to raise the penopubic junction to the level of the pubic symphysis must be estimated. 2. The volume of pubic and inguinal fat should be assessed. 3. The examiner determines whether sufficient healthy penile skin is present with an erection when the penopubic level is raised to the pubic symphysis. 4. The existence of glans and penile skin inflammation, phimosis, or tight penile skin is evaluated. 5. The presence of a penoscrotal web is noted. 6. The examiner assesses whether firm attachments are present from the ventral Buck’s fascia to the dartos fascia at the penoscrotal web. 7. Any significant hydrocele is documented. 8. The surgeon determines whether an abdominoplasty or excision of a large abdominal panniculus may be needed. Most patients with massive weight loss will have sufficient penile skin for shaft coverage unless severe inflammation has been long-standing or a previous overly aggressive circumcision was performed. Surgical goals are to elevate the pubic skin, to remove excess pubic and inguinal fat without leaving an unsightly concavity, and to firmly attach the dorsal and ventral penile skin to the corporeal bodies with tacking sutures. An abdominoplasty can be performed at the same time but is optional and usually unnecessary. A panniculectomy may need to be done during the same procedure to prevent an unsightly overhanging shelf of skin and fat. The patient is shown the probable postoperative appearance in front of a mirror while he is standing. This will help him to develop realistic expectations of what can and cannot be accomplished through surgical intervention. Informed consent is obtained. It is helpful to use a team approach, consisting of a urologist and a plastic surgeon. The urologist can assist with genital anatomy, help to create a pharmacologic erection, and correct a significant hydrocele. However, almost all urologists have a poor understanding of the pathophysiology or surgical treatment of a buried penis. The plastic surgeon should be the primary surgeon, especially when dealing with the pubic region and with penile skin coverage. If the patient has had a previous abdominoplasty or pubic lift and has adequate penile skin, he may still have a buried penis without ptotic pubic skin or pubic fat excess. In such a case, the buried penis is caused by lack of attachments of the Buck’s fascia and tunica albuginea to dartos fascia and skin. Correction involves tacking of the subdermal tissue of the penopubic junction to the tunica albuginea through a small transverse incision just above the penopubic junction, along with penoscrotal tacking. If the penoscrotal tacking is not performed, there will be a significant recurrence rate. Pubic liposuction is usually also performed. A patient with chronic skin irritation, phimosis (tight cicatrix), or relative tightness should be treated with a several-week course of a strong steroid cream such as clobetasol propionate 0.05% cream. The cream may loosen a cicatrix or improve skin quality enough in some cases to salvage adequate penile skin, so that skin grafts or scrotal flaps can be avoided. If a phimosis is present or if the skin cannot be pulled back enough to expose the glans or shaft, evaluation of skin adequacy is determined during surgery. Usually penile skin inflammation will improve postoperatively once chronic dampness is corrected with hidden penis surgery. A large hydrocele should be corrected during surgery to take tension off the penoscrotal tacking sutures. A penoscrotal web should be eliminated to give the patient more functional penile length. The pubic area is infiltrated with lidocaine with epinephrine. The patient should be evaluated standing in front of a mirror, sitting to see whether further burying occurs, and lying down. While the patient is standing, the surgeon pushes in the skin at the penopubic junction down to the rectus fascia and pushes in the ventral skin at the penoscrotal junction. This maneuver simulates the postoperative result, helps determine the amount of pubic skin that needs elevation, and helps to judge the adequacy of penile skin. A transverse crescent incision is marked just below the panniculus line. At least 7 cm of escutcheon is left to produce a normal appearance. Pubic skin will tend to retract once fat is removed, so care must be exercised not to overestimate the amount of skin to be removed. The incision length is determined by the amount of skin removal required to raise the escutcheon without causing lateral dog-ears. If an abdominoplasty is not planned, a partial panniculectomy may need to be performed to prevent a steep overhang of excess abdominal skin. The determination of the amount of panniculus skin to be removed is usually made during the procedure. On rare occasions in a massive-weight-loss patient, bilateral lateral, elliptical, or inverted wedge excisions of lower pubic skin may also need to be performed to eliminate excess horizontal pubic skin. The arms are positioned at 90 degrees on armboards with padding.
Contouring of the Male Genitalia
SURGICAL ANATOMY
BURIED PENIS
Indications and Contraindications
Patient Evaluation
Preoperative Planning and Preparation
Surgical Technique
ANESTHESIA
MARKINGS
PATIENT POSITIONING
TECHNIQUE
Suprapubic Dermatolipectomy With Liposuction and Tacking
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine