div class=”ChapterContextInformation”>
2. Strategy to Monitor Adherence
Keywords
Medication adherenceMedication Event Monitoring System (MEMS®)Multidisciplinary approachDigital healthIntroduction
Outpatient drug therapy can be very cost-effective, but only when the drug itself is effective. Unfortunately, drug therapy failures are common and costly. Even for drugs with the highest cure rates, many patients fail to respond or only respond partially. This can cause multiple patient visits, trial courses with several different drugs and even hospitalisation. The only certain result of ineffective drug therapy is increased cost to the health care system [1].
The single most frequent cause of failed drug therapy is poor patient adherence to their prescribed regimen. The problem of non-adherence is well known since Hipocrates [2]. This long-neglected problem has been put into light by the WHO report in 2003 [3]; more than half of patients on long-term regimens fail to take prescribed medications correctly. But medication adherence problems are difficult to identify and treat, because patients with suboptimal adherence are tough to distinguish from truly nonresponsive patients. Nonadherence is also a problem when making critical dose level determinations and when titrating patients onto drug therapy. Poor adherence can lead to unnecessary testing, added therapy, and avoidable admissions.
Effective management of adherence can simplify clinical management and improve patient care, while at the same time minimizing negative outcomes and helping to lower total costs. The benefits of good adherence are particularly true with “crucial medications”, drugs for which good patient adherence is essential to avoid serious negative therapeutic outcomes. Even for less crucial medications, good adherence equates with better, more cost-effective patient care. Patient adherence to medications requires special attention during the initiation of drug therapy, and it deserves support for effective long-term drug therapy. The WHO stated that “Increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than any improvement in specific medical treatments” [3]. Crucial to the study and management of any phenomenon, biomedical or otherwise, is the ability to make reliable and rich measurements.
The ABC Taxonomy for Medication Adherence
- (A)
“Initiation ”—when the patient takes the first dose of a prescribed medication—is typically a binary event (patients either start taking their medication or not in a given time period).
- (B)
“Implementation ”—the extent to which a patient’s actual dosing corresponds to the prescribed dosing regimen, from initiation until the last dose is taken—is a longitudinal description of patient behavior over time, i.e. their dosing history.
- (C)
“Persistence ”, —the time elapsed from initiation, until eventual treatment discontinuation (i.e. time to event); after discontinuation, a period of non-persistence may follow until the end of the prescribing period. (Fig. 2.1)
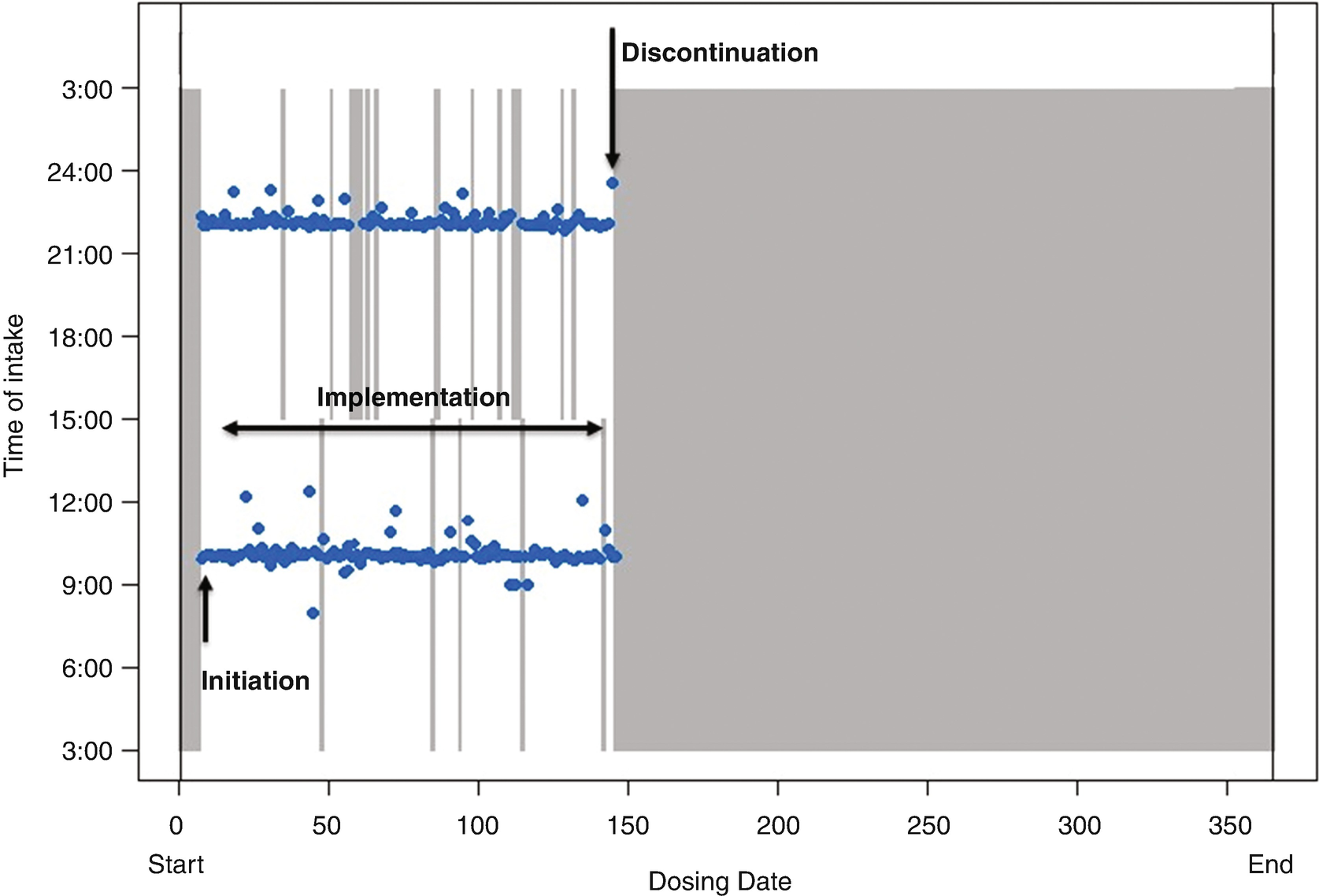
Chronology plot of one case study to illustrate the taxonomy of medication adherence. Relative date from study start is shown on the horizontal axis, and 24-h clock time is shown on the vertical axis. Blue dots indicate the dates and times of drug intake. Grey bars indicate missed doses. Patient is on a twice-daily dosing regimen. The key elements of medication adherence are indicated with black arrows
Non-adherence to medications can thus occur in the following situations or combinations thereof: late or non-initiation of the prescribed treatment, sub-optimal implementation of the dosing regimen or early discontinuation of the treatment. Over 700 determinants are associated to at least one element of non-adherence [5]. While often reported as statistically significant, their predictive value for an individual patient remains very poor [6].
In the field of dermatology, with numerous different skin conditions and a variety of therapies and treatment formulations/instructions, correct adherence to treatment is essential to obtaining optimal efficacy and safety outcomes [7].
Measurement of Medication Adherence
An apt quantification of adherence to medications constitutes the basis for sound adherence management.
Conventional methods for estimating missed doses, such as counting returned medications, or weighing returned cream tubes, don’t indicate when doses are missed. More importantly, they are subject to upward bias by prevalent discarding or hoarding of untaken doses, i.e. some patients simply discard unused medications to please their study investigators or health carers. Clearly and self-evidently, any quantitative analysis that depends on human recall is a priori doomed to imprecision. It is doubtful that any individual could accurately recount information about the medication s/he took weeks prior, and further doubtful that s/he could recall what was forgotten.
Reliance on pill-count data or patient self-reported adherence is responsible for consistent overestimation and prevalent misunderstanding of patients’ non-adherence in clinical trials and in medical practice.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


