div class=”ChapterContextInformation”>
7. Adherence in Psoriasis
Keywords
PsoriasisAdherenceTopical treatmentCorticosteroidsVitamin D analogsCalcineurin inhibitorsBiologicsMethotrexatePhototherapyIntroduction
Psoriasis is a chronic, immune-mediated skin disease that affects up to 3% of the world population and more than eight million Americans [1]. Regardless of psoriasis severity, nearly 60% of psoriasis patients consider to have a major effect on their quality of life (QoL) [2]. Recent studies provided evidence that psoriasis is a systemic disease with multiple cardiovascular and metabolic comorbidities [3]. Patients experience a negative impact on their physical, emotional, and psychosocial well-being. Many psoriasis patients experience embarrassment, self-consciousness, depression, and may suffer from social isolation [2]. Likewise, the economic burden of psoriasis is high. A systematic review estimated that in 2013, direct psoriasis costs ranged from $51.7 billion to $63.2 billion, the indirect costs ranged from $23.9 billion to $35.4 billion, and medical comorbidities were estimated to cost $36.4 billion [4].
Management of psoriasis can be as complex as the disease itself and should be based on the type and severity of psoriasis. Treatment may involve topical corticosteroids, topical steroid-sparing agents such as vitamin D analogues, retinoids, and tacrolimus, phototherapy, and oral therapy with systemic agents such as methotrexate (MTX) and cyclosporine, or treatment with biologic agents. Multifaceted treatment approach may be required to manage complicated disease. However, the complexity of such treatment plans may hinder treatment adherence. Up to 40% of patients self-report that they do not take their medication as directed [5, 6]; moreover, self-report tends to underestimate true non-adherence rates. A 10% decrease in adherence can correspond with a worsening of psoriasis by one point on a nine-point scale [7]. Since nonadherence may explain suboptimal treatment responses, a solution may be to assess and improve adherence prior to escalating therapy.
Higher rates of adherence correlate with improved clinical response. Bettering treatment adherence has the potential to considerably improve treatment outcome as well as patients’ QoL and possibly help control the systemic effects as well. This chapter will assess the prevalence of nonadherence in psoriasis patients, look into nonadherence associated with various treatment modalities, discuss barriers to adherence, and suggest interventions, which may improve psoriasis treatment adherence.
Prevalence of Nonadherence in Psoriasis
Prevalence of nonadherence in psoriasis
Study | Sample size | Psoriasis treatment evaluated | Measure of adherence | Key results |
|---|---|---|---|---|
Zaghloul et al. [10] | N = 201 | Topical and oral treatment | Pill count and medication weight of topical therapy were used to objectively measure medication adherence. | The overall mean medication adherence was 60.6% |
Carroll et al. [15] | N = 30 | Topical therapy | Adherence was measured using 3 methods of adherence monitoring: electronic monitoring caps; medication logs; and medication usage by weight. | Adherence rates calculated from the medication logs and medication weights were consistently higher than those of the electronic monitors (P < 0.05). Electronically measured adherence rates declined from 84.6% to 51% during the 8-week study (P < 0.0001). |
Storm et al. [9] | N = 86 | Topical and oral treatment | Patients were searched using EMR and looked up in the national electronic pharmacy register. | 44.2% (N = 38) of psoriasis patients failed to pick up their prescription. |
Lynde et al. [48] | N = 75 | Narrow-band UVB phototherapy | Adherence was measured by monitoring if patients followed up tor receive their narrow-band UVB phototherapy treatment | Only 21.6% of patients were adherent 80% of the time to phototherapy sessions. |
Esposito et al. [38] | N = 650 | (TNF)-α blockers, acitretin, and cyclosporine | Data was collected from digital databases and/or medical records. | Retention rate, the proportion of patients who maintain the same drug in a given time period, at month 24 was 81.4 (±3.2) for (TNF)-α blockers compared to methotrexate (61.5% ± 4.3), acitretin (52.2% ± 1.0), and cyclosporine (28.6% ± 2.7). |
Doshi et al. [39] | N = 2707 | Biologics (adalimumab, etanercept, infliximab, and ustekinumab) | Analysis was performed using Medicare Chronic Condition Data Warehouse files | During the 12 month follow-up, 38% of patients on biologics (adalimumab, etanercept, infliximab, and ustekinumab) were adherent and 46% discontinued treatment. |
Alinia et al. [16] | N = 40 | Topical fluocinonide | Adherence was measured using electronic monitoring. | In the first month, no medication was used on 37.4% of the days; over the last month of treatment (month 12), no medication was used on 50.9% of the days. Drug holidays of 7 days or more without using treatment were common, occuring in 35.2% of subjects in the first month and 42.8% in the 12th month of study. |
Dommasch et al. [34] | N = 22,742 | Adalimumab, etanercept, ustekinumab, acitretin, and methotrexate | Adherence was measured by using a proportion of patients, dichotomized as adherent (≥0.80) or nonadherent (<0.80). | Among new users of systemic medications, adherence to adalimumab, etanercept, and ustekinumab was greater and acitretin lower compared with methotrexate. |
Psoriasis patients had the lowest rate of primary adherence compared to other chronic dermatologic conditions, with 44% of psoriasis patients failing to fill their prescriptions [9]. In a study assessing adherence to both topical and oral psoriasis treatments, mean medication adherence was 60.6% when assessed by pill count and medication weight while self-reported adherence rates by patient interview were 92.0%. [10] Both self-reported measures and medication weights tend to overestimate adherence rates compared to electronic monitoring [6]. Electronic monitoring may consists of a microchip installed into the medication cap to record the opening and closing of the bottles. Electronic monitoring measured an adherence rate of 67% compared to 92% as recorded by psoriasis patient diaries [11].
Adherence rates also vary widely depending on treatment modality. In a self-reported questionnaire, adherence rates were 100% for biologics, 96% for oral medications, 93% for phototherapy, and 75% for topical therapies; however, these rates are likely inflated given that the measurements were self-reported and subjective [12].
Nonadherence to Specific Treatments
Nonadherence to Topical Treatments
Topical treatments are associated with the lowest adherence rates. While 77% of surveyed patients reported nonadherence overall, topical treatments had the highest nonadherence rate (97%), with lack of treatment efficacy cited most frequently as the reason for nonadherence [13]. A systematic review on adherence to topical psoriasis treatments showed frequency of applications varying between 50% and 60% of those expected. Patients also applied between 35% and 72% of the prescribed dose [14]. Long-term adherence rates are even lower compared to short-term rates. Adherence to topical psoriasis medications decreased from 84.6% initially to 51% at the end of the 8 weeks [15]. In a study using electronic monitoring of topical treatment over the course of 12 months, patients used no treatment 37.4% of the days in the first month. By the twelfth month, patients used no treatment to 50.9% of the days. Drug holidays of 7 days or more were common, with a rate of 35.2% of subjects in the first month, increasing to 42.8% of subjects in the twelfth month [16].
Low adherence rates are similar between different topical treatments—50% with topical steroids, 57% with vitamin D derivatives, 41% with salicylic acid agents [14]. Commonly cited reasons for poor adherence to topical treatments include low efficacy, increased time consumption with application, and poor cosmetic characteristics of the specific preparation. Similarly, a patient survey conducted on 1291 psoriasis patients throughout Europe found that reasons for nonadherence included poor cosmetic characteristics (29%), low efficacy (27%), increased time consumption (26%), and occurrence of side effects (15%) [17]. Slow absorption (44%), increased application frequency required (41%), staining of clothes (34%) and bedding (27%) were reasons frequently cited in a review of topical medication adherence [18]. In another patient survey conducted on 103 Turkish patients, respondents felt they were too busy (25%), fed up (22%), inadequately educated about the disease and its treatment (20%), forgetful (9%), or treatments were too costly (5%) [19]. In a small survey of 50 Korean patients, 18% of patients felt that their topical treatment was moderately or very unpleasant because of its cosmetic characteristics (e.g. odor, texture), 40% considered their treatment to be costly, and 40% were concerned about the adverse effects of treatment. 81.8% of patients cited forgetfulness as the primary reason for nonadherence, 18.8% cited unclear instructions, and 10% reported inconvenience and concerns about side effects [20]. Adherence improved with higher efficacy treatments, treatments that were less greasy, sticky, or smelly, and treatments with a lower risk of side effects [14].
Topical Corticosteroids
Even though topical corticosteroids are the mainstay of topical psoriasis treatment, patients may hesitate to use them. In a patient questionnaire on adherence to topical corticosteroids in psoriasis patients, 60% of respondents were fearful of side effects and 42% reported avoiding prescription medications unless they felt it was absolutely necessary. Similar to the reasons for nonadherence to topical treatments overall, efficacy, time, formulation, and cost all contributed to low adherence to topical corticosteroids, with 15% of patients surveyed attributing their nonadherence to the product being “too messy/oily/sticky” and 10% citing increased frequency of application required through the day [21]. Dissatisfaction with efficacy, inconvenient or unpleasant treatment, undesirable cosmetic properties (e.g. greasy, desiccating, sticky, or smelly vehicles), and fear of adverse drug effects were common reasons for nonadherence to topical corticosteroids repeatedly cited in multiple studies [12, 14, 17, 22, 23]. Although ointment formulations are more efficacious when applied as prescribed, overall low adherence given the poor cosmetic characteristics and inconvenience with application results in suboptimal treatment outcomes [24]. Different formulations, such as foams and sprays, are more likely to have greater patient acceptance, consequently translating to greater adherence and improved treatment outcomes. Prices of topical corticosteroids, including generic preparations, are dramatically rising—a single tube of product can cost several hundred dollars. Significantly increasing cost of treatment is also likely to contribute to nonadherence [25].
Vitamin D Analogues
Topical vitamin D analogues for treatment of psoriasis are as effective as mid-potency corticosteroids and include calcipotriol, calcitriol, and tacalcitol. Skin irritation is a commonly reported side effect. In a randomized, single-blinded study involving 75 psoriasis patients comparing the safety and efficacy of calcitriol and calcipotriol, calcitriol was associated with decreased rates of perilesional erythema and edema, stinging, and burning. Irritant and contact dermatitis were adverse effects only seen in patients treated with calcipotriol [26]. Combined use of topical vitamin D analogues and corticosteroids is more effective than either agent alone; the anti-inflammatory effects of the topical corticosteroid reduce the irritation caused by the vitamin D analogue, while the vitamin D analogue acts as a corticosteroid-sparing agent and reduces corticosteroid-specific side effects [27]. Calcipotriol-betamethasone dipropionate compound therapy was more effective and better tolerated than either placebo, calcipotriol, or betamethasone alone. Patients in the study reported ease of use (95.2%), good skin absorption (77.7%), good cosmetic characteristics of the vehicle (74.3%), decreased time consumption (73.4%), and little interference with social activities (68.4%) as reasons for adherence [28].
Calcineurin Inhibitors
Calcineurin inhibitors are effective for treatment of psoriasis in sensitive areas and include topical tacrolimus and pimecrolimus. Both medications are generally well-tolerated; the most common side effects reported include burning, stinging, hyperesthesia, and itching [29]. There is a FDA-issued black box warning based on a theoretical risk of lymphoma and skin cancer with topical calcineurin inhibitor use. No definite causal relationship has been established and further studies have not found any evidence of an associated increased risk of malignancy; however, this may decrease adherence rates as fear of adverse effects is a commonly cited reason for nonadherence [30].
Tazarotene
Tazarotene , a topical retinoid, is an effective treatment option for psoriasis; however, its use is limited by its adverse effects, including pruritus, burning, stinging, erythema, irritation, dermatitis, and desquamation [31]. Concomitant treatment with a topical corticosteroid reduces irritation and can improve adherence rates [32].
Tar
While not a first-line therapy for psoriasis, tar-based treatments can be a helpful adjunct to topical corticosteroids. Many patients, however, do not find tar-based treatments to be cosmetically acceptable and often find products to be messy with an unpleasant odor. Topical tar preparations can also stain hair, skin, and clothing [33].
Nonadherence to Systemic Therapies
Moderate-to-severe psoriasis frequently requires long-term systemic therapy. As with topical treatments, multiple factors such as efficacy, safety, and patient’s overall satisfaction with treatment affect adherence. A recent retrospective, comparative cohort study studied adherence of new users of acitretin, adalimumab, etanercept, MTX, and ustekinumab using a large US health insurance claims database. Among the 22,472 new users of systemic medications, adherence to adalimumab, etanercept, and ustekinumab was greater and acitretin lower compared to MTX [34]. These results were consistent with prior studies using data outside US, which have shown greater adherence to biologics compared to other systemic agents [34].
Drug survival may also serve as an indicator of therapeutic success. A study assessing drug survival rates and reasons for discontinuation demonstrated that the crude probability for drug survival in patients with moderate-to-severe psoriasis was higher for biologics (ustekinumab, followed by adalimumab, etanercept, infliximab) than of traditional systemic therapies (MTX, acitretin, and cyclosporine A). Inefficacy with respect to cutaneous lesions was the reason for discontinuing biologics with the exception of infliximab, which along with traditional systemic antipsoriatic agents, were most frequently discontinued to adverse events [35]. A study looking at retention rate, the proportion of patients who maintain the same drug in a given time period, revealed that global retention rate of (TNF)-α blockers at month 24 was 81.4% (±3.2) compared to MTX (61.5% ± 4.3), acitretin (52.2% ± 1.0), and cyclosporine (28.6% ± 2.7) [38]. Long-term treatment of psoriasis patients should integrate the current knowledge of drug survival rates when making therapeutic decisions.
Biologics
Psoriasis patient adherence to biological treatments is challenging. Psoriasis patients appear to have the highest adherence with biological therapy. In Medicaid-enrolled patients, adherence rates were highest for biologics (66%) compared to other psoriasis treatments which included topical, oral/systemic agents, and phototherapy (36%) [36]. The overall pharmacy claim rates for biologics were 61.9% compared to 50.7% for MTX [34]. Injectable drugs are often preferred over orally administered medicine [37]. This may contribute to increased adherence of injectable biologics compared to oral medications. Positive feedback on adherence due to the high efficacy of biologics in psoriasis patients may contribute to the long-term adherence to these drugs. Patients on biologics also usually suffer from a more severe form of psoriasis compared to patients using topical therapy or phototherapy. In theory, this might result in higher motivation and hence treatment adherence among those on biologics, but patients with more severe psoriasis may have worse adherence than those with milder disease [10, 12]. Drug survival time was also longer for biologics than for oral agents [35]. In a retrospective study, biologics targeting tumor necrosis factor (TNF)-α had a 72.6% adherence rate after 30 months of treatment [38].
However, psoriasis patients continue to have poor adherence to biologics . In a retrospective claims analysis of 2009 through 2012 data from Medicare patients, 2707 patients initiating adalimumab (40%), etanercept (37.9%), infliximab (11.7%), and ustekinumab (10.3%) were examined. During the 12-month follow-up, 38% of patients were adherent and 46% discontinued treatment [39]. In another study, ustekinumab had a higher adherence rate compared to other biologic agents. In biologic-naïve and biologic experienced psoriasis patients, the drug survival of ustekinumab was better than adalimumab and etanercept [34]. Better adherence to ustekinumab was also supported by an Australian study on the use of biological therapies in psoriasis in real-life clinical setting; approximately 90% of patients remained on ustekinumab treatment after almost 3 years [40]. Reasons for nonadherence to biologics may include fear of side effects and high cost of treatment.
Methotrexate
In psoriasis, MTX is an anti-inflammatory medication; it increases endogenous anti-inflammatory adenosine levels. MTX is effective for psoriasis. Approximately 40% of patients on MTX achieve 75% improvement in Psoriasis Area and Severity Index (PASI 75) if provided as continuous therapy over 4-month period at reasonable dosing [41]. Although an effective medication for psoriasis, the efficacy of MTX is lower compared to most biologic agents. Severe adverse events such as pancytopenia, hepatotoxicity, and pulmonary fibrosis and less serious side effects such as nausea and vomiting may occur with MTX therapy [41]. Fear of potential side effects may contribute to nonadherence to MTX.
Few studies have examined the overall adherence of MTX in psoriasis patients. A study looking at retention rate revealed that retention rate for MTX was lower than that of TNF-α blockers at 24 and 30 months (p < 0.001) [42]. There is also a difference between adherence to oral and subcutaneous (SC) MTX. To further investigate this, one study assessed the adherence of SC MTX in a multicenter retrospective analysis of chronic plaque-type psoriasis patient registry. Adherence to self-administered SC MTX after 6 months of treatment was high. Most patients who were switched to SC MTX after an unsuccessful treatment with oral MTX remained on subcutaneous regimen [43].
Cyclosporine
Dermatologists may use cyclosporine to treat extensive or disabling psoriasis when rapid response is desired. In psoriasis, cyclosporine works by blocking interleukin (IL)-2 and other proinflammatory cytokines and by preventing T-cell activation. Better treatment response is seen in patients receiving highest dosage, and higher doses are also related to increased risk of renal toxicity, hypertension, and intolerability [41].
Although cyclosporine is more useful as a rescue drug than long-term psoriasis treatment, fear of side effects may cause suboptimal adherence even with short-term use. Retention rate of cyclosporine at months 24 and 30 was also lower than retention rate of TNF-α blockers (p < 0.001) and discontinuation was mainly due to intolerance, which was also true for conventional drugs MTX and acitretin [42].
Acitretin
Acitretin is the most widely used retinoid in psoriasis treatment and effective both as monotherapy and combination therapy with conventional systemic drugs as well as biologics. As monotherapy, it’s highly efficacious in specific clinical subtypes of psoriasis such as erythrodermic psoriasis, palmoplantar psoriasis, and nail psoriasis [44]. In a study evaluating factors associated with drug survival of MTX and acitretin in patients with psoriasis, younger age (p < 0.001) and psoriatic arthritis (p < 0.001) were factors associated with treatment dropout [45]. Acitretin lacks immunosuppressive side effects; the side effects are usually mild and can be minimized with dose titration [44]. These features of acitretin may help patients better adhere to the treatment.
Nonadherence to Light Therapy
Phototherapy is frequently used to treat plaque psoriasis as it is effective, safe, and accessible treatment without any systemic side effects [46]. It counteracts inflammation-induced characteristic pathological changes of psoriasis because ultraviolet radiation induces apoptosis in T-lymphocytes and in keratinocytes in the epidermis. Ultraviolet-B (UVB) treatment is also highly cost-effective [47] which may aid in adherence to treatment. However, use of UVB phototherapy in the office setting can be challenging for patients. Office-administered UVB requires psoriasis patients to visit two to three times per week for 15–25 treatments, which can be a burden for patients. Hurdles include patients taking time off of work, arranging transportation, and paying co-pays. Therefore, it is no wonder that only 21.6% of patients were adherent 80% of the time to phototherapy sessions [48].
A study of moderate-to-severe psoriasis patients assessed adherence to oral acitretin and home UVB therapy over a 12-week period. Patients had better adherence to home UVB therapy than oral acitretin. Easier access and high perception of effectiveness of home phototherapy (96% of patients reporting positive results) may have contributed to the improved adherence of this treatment [49, 75]. Patients treated at home have a lower burden of treatment and evaluate their therapy more positively than patients treated in the outpatient department (P values ≤0.001) [76]. Lower burden could contribute to better adherence to home treatment [77]. In a retrospective observational study conducted to evaluate patient’s adherence to a prescribed three-times-per-week treatment protocol of home UVB phototherapy for localized psoriasis, adherence was calculated for each patient by dividing the number of treatments the patient administered by the number of treatment opportunities they had. Among the 18 psoriasis patients, median continuous adherence was 81% [78].
Barriers to Adherence
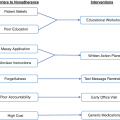
In a series of patient interviews, there were several major themes that emerged surrounding the issue of nonadherence in psoriasis. Patients often perceived psoriasis and its treatment as a burden and social stigma, limiting their ability to engage in social activities and balance their work commitments. Poor control of symptoms and unpredictable response to treatment in addition to the perception of psoriasis as a lifelong chronic condition worsened adherence by causing psychological stress and feelings of frustration and hopelessness. Patients often did not feel empathy from healthcare providers and felt that providers rarely acknowledged the challenges associated with medication use. There is some degree of bias in these responses, however, as patients were recruited from psoriasis support groups [50]. Primary drivers of poor adherence in the treatment of skin conditions overall include a poor doctor-patient relationship, lack of knowledge about the disease and treatment, lack of belief in the treatment, unrealistic expectations, side effects or fear of side effects, messy and complex treatment regimens, inadequate follow-up, forgetfulness, psychosocial factors, and cost [51]. Barriers impacting adherence to psoriasis range from education, perception of treatment effectiveness, poor communication, forgetfulness, and poor accountability as well as high cost of treatment.
Fears of Adverse Effects
In a study assessing adherence to conventional systemic and biologic therapies in a real-world setting among psoriasis patients, factors associated with intentional nonadherence included being on conventional systemic therapy, having strong medication concerns, weaker routine for taking their systemic therapy, and long treatment duration. Overall 22.4% of patients out of the total sample (N = 811) using self-administered systemic therapies were classified as non-adherent [50]. Another study surveying physicians and psoriasis patients determined that inconvenience and concern about side effects were common reasons for topical treatment discontinuation. More than 40% of total patients (N = 50) surveyed were moderately or very concerned about side effects of topical treatment [20]. Adequately assuring patients about the safety of the drug and explaining that the large majority of patients do not experience the rare side effects may be one approach to address this.
Poor Communication and Knowledge Gaps
The survey study of psoriasis patients using topical treatments also determined that more than 15% of patients did not get enough information about the drug although the majority were satisfied with the length of consultations [20]. This may indicate the possibility that the information was shared with the patients, but it was not sufficient or the patients did not necessarily understand the information conveyed to them and had unanswered questions. Helping patients have a better understanding of their medicine may improve treatment adherence. Another study exploring perceptions of psoriasis patients on their disease and its management revealed that medication underuse was caused by concerns about potential side effects, perceived poor control of symptoms, and feelings of anxiety [50]. Inadequate knowledge about the disease and therapy was listed as a reason for missing treatment by 20% of 103 psoriasis patients in a different study [27]. These findings highlight the importance of patient education and good communication between patients and their physicians.
Forgetfulness
Forgetfulness is a common cause of unintentional nonadherence among psoriasis patients as in many other diseases requiring long-term treatment [27, 52]. Useful strategies to address this problem may include reminders such as text messages or phone calls [53]. Having nurses and other healthcare staff more involved with psoriasis patients may help improve treatment adherence by helping with treatment reminders and also being available to instruct patients on how to apply medications and providing important information about disease when patients have develop questions [54].
High Medication Cost
Increasing costs of psoriasis treatment may also contribute to suboptimal adherence. Biologics are an essential part of treatment regimen for many patients suffering from psoriasis. However, this treatment modality may be very costly [55]. In a large, multinational, population-based survey of psoriasis and psoriatic arthritis patients in Europe and North America involving 3426 subjects, 11% of patients attributed cost/insurance reimbursement issues as the reason for their discontinuation and secondary nonadherence [56]. Low income has a negative impact on adherence as patients may not be able to afford expensive medications [57]. Making medications more affordable and patient assistance programs that provide financial support may be solutions to help combat this adherence barrier.
Adherence Interventions for Psoriasis
Studies reporting adherence intervention in psoriasis patients
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


