div class=”ChapterContextInformation”>
1. Reasons for Nonadherence
Keywords
NonadherenceHealthcare providerPatientReasonsBarriersIntroduction
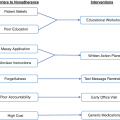
Poor patient adherence is especially challenging in the field of dermatology, where only 50% of patients with chronic skin conditions adhere to the treatment plan outlined by their provider [1]. About one-third of patients never redeem their prescriptions from a dermatology clinic. Even if patients do fill the prescriptions, adherence often drops off after a few days. Poor adherence leads to poor health outcomes and increased financial expenditure for patients. By recognizing and addressing common barriers to treatment adherence, providers may help patients successfully incorporate and adhere to treatment regimens. Improving patient adherence may provide a convenient way to improve patient outcomes and decrease healthcare costs.
While there are various reasons for nonadherence, one conceptual model of barriers to adherence focus on patient, prescriber, and healthcare system factors [2]. Nonadherence can also be categorized into three phases: initiation, implementation, and persistence. Initiation includes failure to fill and begin taking a prescription [3]. Implementation is the patient’s ability to agree, comprehend, and translate the healthcare provider’s instructions. Finally, persistence involves maintaining the recommended treatment regimen [3, 4].
This chapter will first discuss barriers specific to patients, providers, and healthcare systems, then it will discuss common barriers that are shared between patients and providers.
Patient-Centered Barriers
Intentional | Unintentional |
|---|---|
Patient beliefs | Forgetfulness |
Fear of adverse effects | Lack of health-related education |
Patient preference | Psychiatric illnesses |
Complex treatment regimen | Poor communication |
Medication cost | Failure to refill medication |
Insurance difficulties | Limited access to healthcare |
Poor patient-physician relationship | Poor patient-physician relationship |
A patient’s beliefs can influence whether they initiate, implement, and persist with therapy. A patient may believe he received the wrong diagnosis, and therefore wrong medication, from his provider. If a patient feels he was not adequately examined and understood, he may be less likely to fill or take the suggested medication. A patient might also believe his condition is only temporary, and therefore prematurely stop therapy after some improvement. This can be especially challenging in chronic conditions that require continuous treatments [10].
A common reason for intentional nonadherence is a patient’s fear of adverse effects due to the medication [11]. “Steroid phobia” describes negative feelings and beliefs about using topical corticosteroids. Common concerns about topical corticosteroids include skin thinning, the potential of topical corticosteroids to affect growth and development, and nonspecific long-term effects [12]. In one study, prevalence of steroid phobia in caregivers of children with atopic dermatitis (AD) reached about 38% [12]. If patients or caregivers fear of the topical corticosteroid side effect profile, they may be less willingness to use the medication as prescribed.
Patient preferences can impact adherence; therefore, a patient-centered approach may be helpful. Addressing and reconciling patient goals and preferences can help providers and patients agree on a feasible treatment regimen [13]. For example, some patients with severe psoriasis may prefer oral over injectable medications, even if the injectable medication is more likely to result in better disease control. Patient preference of a particular vehicle formulation for their topical medication may also impact their level of adherence [14, 15]. Subjects satisfied with their prescribed medication are more adherent than unsatisfied subjects (P < 0.001) [16].
Prescriber-Centered Barriers
Patient-centered barrier | Prescriber-centered barrier | Healthcare-centered barrier |
|---|---|---|
Forgetfulness | Complex treatment regimen | Limited access to healthcare |
Psychiatric illness | Prescribing high cost medications | Restricted formularies |
Patient beliefs | Poor communication | Medication cost |
Fear of adverse effects | Switching formularies | |
Patient preference | Copayments |
The high cost of prescription drugs means many patients cannot afford their medications. Patient may fail to pick up their medications, skip doses to make the medication last longer, or stop treatment early due to the cost. However, providers are often unaware how much medications will cost patients. Providers and patients often fail to seek out pricing information before filling prescriptions. Prescribing generic prescriptions increases the likelihood that the patient can afford a medication [17].
Complex treatment regimens often confuse patients and decrease their motivation, leading to poor adherence. Prescribing multiple medications after one office visit or adding prescriptions on top of a large list of medications, can reduce patient adherence. Simplifying treatment regimens reduces the burden of treatment and increases the likelihood that patients will adhere. Patients are more likely to follow a once daily treatment compared to twice daily. Combination medications also reduces the burden of treatment and increases adherence [11, 18, 19].
Poor communication by the provider to the patient can also result in poor adherence. Providers may not adequately explain the patient’s condition, the need for medication, treatment expectations, and potential adverse effects. Patient education is be a key component of the clinical encounter. It offers an opportunity to address patient concerns and build a strong patient-provider relationship. By failing to communicate basic information, healthcare providers may jeopardize a patient’s disease and treatment understanding and overall adherence [11, 20, 21].
Prescribers who fail to create a strong bond with their patient may increase the risk of nonadherence. Using a patient-centered approach may strengthen trust between both parties and prevent a poor patient-provider relationship [11, 22–24].
Healthcare-Centered Barriers
Healthcare-associated barriers to adherence include limited access to healthcare, restricted formularies, switching to a different formulary, and high costs for medications, copayments, or both [25–27]. The patient, provider, pharmacies, hospitals, insurance, and pharmaceutical companies are all components of the healthcare system [28].
Factor that create poor access to healthcare— including living in an area with poor access, lack of transportation, lack of adequate insurance, financial issues, and absence of other resources— also influence adherence [17, 29]. Other healthcare-associated factors that may influence adherence include extensive waitlist for an appointment with a specialist, lengthy wait time within the clinic, and confusing healthcare referral systems [30–32].
Insurance also has a strong influence on healthcare-associated nonadherence. Insurance issues include difficulty finding in-network healthcare providers, drug plans that do not cover certain prescription medications, and unaffordable copayment [11, 22, 23, 33]. For example, providers may not prescribe the best medication if it does not fall in a patient’s restricted network formulary [34]. Such limitations impact the patient, provider, and healthcare system.
Common Barriers of Patients and Providers
Patient | Provider |
|---|---|
Treatment education | |
Poor health literacy | Poor communication skills |
Beliefs and perception of symptoms | |
Fear of adverse effects | Believing patients are adherent |
Treatment dissatisfaction | Failure to acknowledge patient beliefs |
Forgetfulness | |
Failure to remember regimen | Failure to provide instructions |
Psychiatric illness | |
Depression | Failure to recognize psychiatric comorbidities |
Anxiety | Failure to provide appropriate referrals |
Cost and insurance | |
Lack of insurance | Writing expensive prescriptions |
Expensive copay | Failure to provide patient assistance |
Complex treatment regimen | |
Polypharmacy | Prescribing multiple medications |
Inability to follow instructions | Failure to offer prompt return visit |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


