div class=”ChapterContextInformation”>
6. Adherence in Patients with Comorbidities
Keywords
ComorbidityMultimorbidityAdherencePatient educationCare-coordinationChronic conditionsIntroduction
The association of certain dermatoses and other chronic diseases is complex and multifactorial. Lifestyle factors, impaired health-related quality of life, depression, and therapeutic interventions often confound this relationship. When investigating morbidities in the field of dermatology, psoriasis has received the most attention in the last decades [1]. Epidemiological investigations have largely focused on psoriasis-related conditions such as arthritis, cardiovascular disease, and depression [2]. The search for other comorbidities has now extended to other chronic inflammatory skin diseases, such as rosacea, atopic dermatitis, hidradenitis suppurativa, seborrheic dermatitis, and lichen planus [3–7].
The concepts of multimorbidity and comorbidity have become increasingly important as patients with multiple conditions are becoming the rule rather than the exception. Multimorbidity is the co-existence of two or more chronic conditions [8]. The term comorbidity is now taken to mean a condition with other linked conditions (e.g., diabetes and cardiovascular disease), or when there are conditions that commonly co-exist, (e.g., diabetes and depression). There is greater demand for improving patient outcomes with multiple chronic conditions as health care expenditures are higher in these patients compared to patients with a single chronic disease [8, 9]. One in four American citizens lives with two or more chronic conditions [10]. The prevalence of multimorbidity is estimated to be between 25–55% at 60 years of age and 80% in those older than 75 years [11]. Individuals with multimorbidity are more likely to be admitted to hospital, have longer hospital stays, experience depression, and die prematurely [12, 13]. Nonadherence is highly prevalent in patients with multimorbidity, especially when multiple medications are prescribed for each chronic condition [14].
Despite the increasing number of patients with multiple chronic conditions, evidence on the effectiveness of interventions to increase adherence and improve outcomes in such patients is limited. Whereas different interventions for managing chronic disease have been created, these strategies usually focus only on a single disease [15]. We know very little about the potential impact of interventions for improving adherence in patients managing multiple diseases. This chapter will explore what factors act as barriers to medication adherence in patients with multimorbidities. We also aim to evaluate what interventions may enhance patient adherence to treatment regimens.
Barriers to Adherence in Patients with Multiple Chronic Conditions
Medication Barriers
Patients with multimorbidities face compounded barriers related to their medication, including limited medication access, high medication cost, regimen complexity, noxious side effects, and medication intolerance.
Medication Cost
Patients taking multiple medications tend to incur higher out-of-pocket medication costs, which influences how many medications a patient can afford [16]. Patients also may be reluctant to take multiple medications, with some patients reporting they reached their limit or threshold for taking medication. Adding one more drug to their regimen may not be financially feasible, as one out of five low-income patients do not fill all their prescriptions because of cost. Likewise, patients reported skipping doses to make their prescriptions last longer [17]. Trust also plays a role in medication adherence, as patients with low trust in their physician are more likely to forgo medicines because of cost pressures [18].
Polypharmacy
Medication management for multiple chronic conditions often results in polypharmacy , leading to an increased risk of drug interactions that may result in hospitalization and death [19, 20]. These effects are more pronounced in economically disadvantaged, minority populations with fewer financial resources [21, 22]. Polypharmacy also suggests an underuse of necessary treatments, low adherence, and partly preventable mortality, particularly in older patients [23].
Regimen Complexity
Complex regimens may have conflicting directions, leading to decreased adherence in patients with multiple comorbid conditions [24]. The more medications a patient is required to organize and remember, the poorer the adherence. Infrequent and irregular dosing schedules increase regimen complexity (e.g., large quantities of pills taken only one or twice a week) and decrease the likelihood of adherence. Increases in the number of medications or the number of doses per day results in decreased adherence [25].
Side Effects
Noxious medication side effects or route of medication (e.g., injection) play a strong role in low patient adherence. Adverse medication interactions are more likely to occur as the number of medications increase, contributing to decreased adherence. Patients may actively choose not to take the medications because of negative side effects due to either a specific medication or interactions between medications. Even with topical corticosteroids, as many as 80.7% of patients reported having fears of adverse effects, and 36% admitted to treatment nonadherence due to concern about steroid-related adverse effects [26].
Provider Barriers
Multiple Physicians
Fragmentation of care is a significant problem for patients managing multiple chronic conditions. The involvement of both primary care and multiple specialists can result in too many healthcare providers prescribing medications, too many pharmacies filling prescriptions, and no sharing of information between those entities or with the patient [27]. As the number of prescribing providers and pharmacies increases, patients are less likely to adhere to a medication regimen [24]. Patients with a greater morbidity burden have a higher use of specialists even for conditions that are normally managed in primary care [28]. Interestingly, when a specialist, not a primary care physician, is prescribing the medications, adherence is higher among patients [24].
Physician-Patient Interactions
The physician-patient relationship can influence a patient’s decision to adhere to medical recommendations. Issues that may strain the physician-patient relationship and lead to nonadherence include expectations for communication and participation during the clinical encounter, misunderstandings between patients and providers, and different agendas that are not met during clinic visits [29, 30]. When patients report suboptimal communication and relationship with their physicians, they may feel intimidated or disregarded, which often makes it difficult for them to follow the doctor’s recommendations. Furthermore, patients report that when their own preferences and goals were not generally integrated into treatment plans, they ended up taking less medication than prescribed [31].
Patient Barriers
Psychiatric Comorbidities
A serious, but often neglected, comorbidity is compromised mental health status . Psoriasis is strongly associated with depression, anxiety, and suicidality [32]. For example, in a recent population-based study, 12.5% of patients with severe psoriasis reported a history of depression, as compared with 4.7% in the control population [33]. Patients with multiple conditions have poorer quality of life, loss of physical functioning, and are more likely to suffer from psychological stress [8, 34, 35]. Mental health disorders, particularly depression, are more prevalent in people with increasing numbers of physical disorders [36]. Patients in whom depression coexists with other medical conditions may be less adherent to medical or behavioral regimens, have more functional impairment, and increased mortality. Patients with psoriasis and depression view the magnitude of treatment benefit as less important compared to patients with only psoriasis. This indifference toward improving their skin condition results in a high risk of nonadherence. In a potentially vicious cycle, nonadherence can result in deteriorated treatment outcome, which might trigger or worsen depression [37]. Although mental disorders often take a back seat to significant multimorbidity, comorbid depression incrementally worsens health compared with depression alone, with any of the chronic diseases alone, and with any combination of chronic diseases without depression [38].
Patient Beliefs
Patients’ beliefs of their conditions and medications influence medication adherence, especially in patients with high comorbidity. Some patients may believe that drugs are toxic products which create a vicious cycle, and that spontaneous recovery may occur without treatment. Patients may consider drug prescriptions to be a consequence of a lack of time or resources for other types of treatments. Some patients have identified the pill burden as an excuse by the health system to not individualize treatment. If patients do not perceive therapeutic effectiveness from their treatment, their motivation could decrease and thus hinder adherence. This is particularly significant in patients suffering from several comorbidities who may require lifelong treatment with certain medications [39].
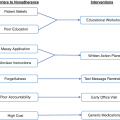
Interventions
Despite the increasing prevalence of patients with multiple chronic conditions, evidence on the effectiveness of interventions to improve clinical outcomes in such patients is limited. Given the complexity of multimorbidity, potential interventions are likely to be complex and multifaceted if they are to address the varied needs of these individuals.
Patient Education
Patient education is the starting point of adherence and nonadherence conduct. Patients’ beliefs and misbeliefs influence both intentional and unintentional nonadherence. Patient beliefs of overmedication, lack of satisfactory results following initial expectations, and a fear of side effects can all lead to nonadherence. Cognitive theories such as health belief model and the theory of planned behavior assume that if patients are educated on the benefits and risks of taking medications, they will be better adherent with the medications [40]. Therefore, health professionals can engage with chronic patients, discuss their health beliefs, and provide them with the adequate information about their illness and treatment to increase adherence.
Education is a central element that enables patients to manage their conditions better. In a focus group about multimorbidity and medication adherence, participants stressed the importance of patient education. Participants reported that more information would improve their adherence to the treatment regimens. A lack of knowledge about the therapeutic mechanism and potential adverse effects increased patients’ fear of medication and distrust in medicine. Patient confidence in the treatment increased when health providers explained how their medications worked. If patients received adequate information, they showed a clear interest in being involved in decision-making throughout the therapeutic process [39].
Care-Coordination Interventions
Clinical guidelines usually focus on a single disease, so management of multimorbidity can be overwhelming for both patients and providers because of overlapping or conflicting treatments. Care-coordination involves organizing different providers and services to ensure timely and efficient health care delivery. Examples of case-coordination interventions include multidisciplinary teams, case management, and health technology. These interventions focus not only on clinical aspects of care, but also consider patients’ health priorities and goals and their social and emotional well-being. In patients with multiple chronic conditions, care-coordination interventions improved cognitive functioning, increased use of mental health services, and reduced symptoms of depression and functional impairment [41].
In dermatology, care-coordination through the use of multidisciplinary clinic practices models have helped provide efficient care have improved outcomes for patients with psoriasis, cutaneous lymphomas, and sarcoidosis [42–44]. The emphasis of care-coordination in dermatology has led to care-coordination as one of the improvement activities considered in the Merit-based Incentive Payment System [45]. While teledermatology has potential to improve care-coordination for patients, fragmentation of care and inadequate follow-up are concerns [46].
Combining educational components with care-coordination interventions appear to have the greatest potential for improving outcomes in patients managing multiple chronic conditions. The combination of case management, education, and self-management significantly reduced depressive symptoms in older adults with multimorbidities. Furthermore, care-coordination or telemedicine interventions with an education component significantly reduced patient disability and improved cognitive functioning [41].
Simplify Regimens
Patients with multimorbidity may have specific problems with medication use that relate to polypharmacy and managing complex treatment regimens. For that reason, interventions targeting specific difficulties related to medication management may be particularly effective. Subjects from the focus group report wanting a therapeutic balance between the dosage schedule and their quality of life. Tailoring treatment regimens to patients’ needs and preferences might improve adherence to medication [39]. Reducing the complexity of drug regimens can improve adherence and clinical improvement for some patients, although most of these studies were conducted with single disease conditions [47]. Polymedicated patients want to prioritize drugs regarded as essential for survival and to maintain a good quality of life. From their point of view, doctors should review their medications regularly to see whether they are still necessary [39].
If the number of medications cannot be reduced, then strategies to make treatment regimens and administration are necessary. Packaging interventions such as pill boxes and blister packaging effectively increase medication adherence [48]. Linking medication taking with existing habits also increase medication adherence. Using prompts, such as text messaging, cell phone alarms, and calendars, have also shown promise in helping patients to learn their regimen and remember to take their medications [49].
Patient-Provider Relationship
Patients often report a good relationship with their doctor as the most significant facilitator for adherence [31]. When patients were asked what helped them to follow a treatment or improve medication adherence, responses centered on the attention they received from their prescriber [39]. Patients who feel that their physicians communicate well with them and actively encourage them to be involved in their own care tend to be more motivated to adhere. The amount of contact a patient has with a physician positively correlates with medication adherence [24]. Higher rates of contact with the medical office staff provide more opportunities for medication management and adherence checks.
The greater the patient’s confidence in the prescriber, the greater the patient’s confidence in the treatment. A strong patient-provider relationship also enhances patient self-care, which in turn improves medication adherence [50]. Many patients report wanting more complete information and education from healthcare providers so as to be more involved in decision-making. When physicians and patients agree on how involved patients should be in their care, adherence is improved [51]. The concept of therapeutic alliance has been largely studied in the field of psychotherapy, where it plays a major role as a good predictor of clinical outcome [52]. It helps both healthcare professionals and patients to work together effectively. The literature has also described the relationship between good medication adherence and therapeutic alliance [53].
Patient participation promotes effective management plans, fosters more effective treatment relationships between patients and providers, and provides the context to explore therapeutic options, discuss medication regimens, and consider follow-up actions [54]. However, patients also complain about the little attention given to mental health status in medical visits. Patients may seek greater clinical support concerning emotional aspects, such as a holistic approach that takes their preferences and family context into account [39].
Treatment of Mental Health Status
It is important to assess the mental health status of patients. Addressing and treating patients’ depression may be a neglected opportunity to improve care. The prevalence of psychological comorbidities with multiple chronic conditions is high, so referral to a psychologist or psychiatrist is recommended if psychopathology is noted. While it remains uncertain whether depression management results in increased treatment adherence, depression management can decrease the morbidity associated with other chronic conditions. Sustained depression management program over at least 2 years can diminish the combined effect of multimorbidity and depression on mortality [55].
Conclusion
Understanding medication regimen complexity and lack of shared decision making seem to be major barriers to adherence faced by patients with multimorbidity. Providers should consider interventions aimed at improving care-coordination, patient education, simplifying treatment regimens, and strengthening the provider-patient relationship to help improve patients’ adherence to complex medication regimens.
Conflicts of Interest
Dr. Feldman is a speaker for Taro. He is a consultant and speaker for Galderma, Abbvie, Celgene, Abbott Labs, Lilly, Janssen, Novartis Pharmaceuticals and Leo Pharma Inc. Dr. Feldman has received grants from Galderma, Janssen, Abbott Labs, Abbvie, Celgene, Taro, Sanofi, Celgene, Novartis Pharmaceuticals, Qurient, Pfizer Inc. and Anacor. He is a consultant for Advance Medical, Caremark, Gerson Lehrman Group, Guidepoint Global, Kikaku, Lilly, Merck & Co Inc., Mylan, Pfizer Inc., Qurient, Sanofi, Sienna, Sun Pharma, Suncare Research, Valeant, and Xenoport. Dr. Feldman is the founder, chief technology officer and holds stock in Causa Research. Dr. Feldman holds stock and is majority owner in Medical Quality Enhancement Corporation. He receives Royalties from UpToDate, Informa and Xlibris.
Dr. Abigail Cline and Dr. Adrian Pona have no conflicts of interest to disclose.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


