(1)
Klinik für Plastische Gesichtschirurgie, Marienhospital Stuttgart, Stuttgart, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-662-49706-7_12) contains supplementary material, which is available to authorized users.
Keywords
Revision rhinoplastyTip revisionOverresection of the LLCPolly-beak deformityBending techniqueScoring techniqueDome division techniqueSplit techniqueBatten graft techniqueSupratip excisionSkin stretch ing12.1 Surgical Principles in Secondary Tip Correction
The principles of tip rhinoplasty are largely the same for both primary and secondary rhinoplasty. However, in revision surgery, a shortage of inner or outer nasal lining frequently limits re-expansion of a foreshortened and/or underprojected tip framework. Although release of the external skin envelope with wide-field dissection may help to recruit additional external lining, a scarred and contractured internal lining is often the limiting factor in nasal re-expansion. In many cases, the nose was initially shortened by resecting portions of the internal nasal lining. Wide undermining alone seldom provides adequate soft-tissue lengthening, and relaxing incisions may be needed to obtain additional length. In stubborn cases, it is often useful to institute soft-tissue stretching exercises in order to pre-expand the nasal soft tissues. This is accomplished by having the patient repeatedly pull downward on the membranous septum, as well as on the outer nose, for 20–30 min daily over a period of at least 3 months. Sustained and repeated stretching will gradually increase soft-tissue compliance and length similar to tissue expansion.
The most common challenge encountered in secondary tip rhinoplasty is overresection of the tip cartilaginous framework—the lower lateral cartilages (LLCs), the nasal septum, or both. Overresection of the LLCs originates from the misconception that a smaller and more refined tip contour will result merely from cartilage excision. Ironically, aggressive cartilage excision will often have the opposite effect, resulting in poor definition, skeletal destabilization, and unpredictable cartilage collapse. In many cases, collapse will result in tip droop and polly-beak formation, further exacerbating the adverse cosmetic consequences.
To restore the overresected tip framework, the LLCs must be strengthened and reshaped using autologous cartilage grafts. In our hands, the preferred material for tip restoration is septal cartilage. Surplus septal cartilage is frequently available following “aesthetic rhinoplasty,” in which the septum remains untouched. We usually thin the stripes of septal cartilage in the area of the intermediate crus with a motor drill so that bending becomes easier (Fig. 12.1). In cases of previous septal cartilage depletion, we prefer autologous rib or ear cartilage as alternatives. Rib cartilage can be easily and precisely contoured using a motorized drill for thinning and smoothing. In younger patients, progressive surgical thinning of the rib graft on one side enables folding of the cartilage without fracture. Folded rib cartilage can be used to replace the nasal domes in reconstruction of overresected tip cartilages (7 see Chap. 4). In contrast, with many older patients or in partially calcified rib specimens, the bending technique often results in unwanted fractures at the domal fold. When fractures are partial, scoring of the adjacent cartilage sometimes permits additional bending to create a suitable dome unit (Fig. 12.2). In contrast, when the fracture is complete, the grafts are managed similar to a vertical dome division (Fig. 12.3). In the occasional patient, the septal cartilage is extremely thick, enabling the distal columellar strut to be split in two and allowing for replacement of damaged nasal domes (Fig. 12.4). When only segments of the lateral crura are missing, these are replaced with batten grafts (Fig. 12.5).
Another problem in revision tip surgery, especially in thick-skinned noses, is insufficient contracture and adhesion of the skin envelope to the underlying skeletal framework. The result is an imbalance in size between the nasal skin envelope and the skeletal framework, ultimately resulting in the formation of dead space and poor soft-tissue definition. To avoid this problem, either the skeletal framework must be increased in size to stretch the skin envelope or the skin envelope must be reduced in size to improve surface contour and definition. Many patients confronted with this dilemma refuse skeletal enlargement because they are seeking a smaller nose. In those cases that result in poor tip definition and/or supratip fullness (often with polly-beak formation), a supratip skin excision can be helpful. A precise midline fusiform excision of full-thickness skin and subcutaneous soft tissue, followed by a subcutaneous closure, is used to enhance tip definition and minimize surface scarring (Fig. 12.6).
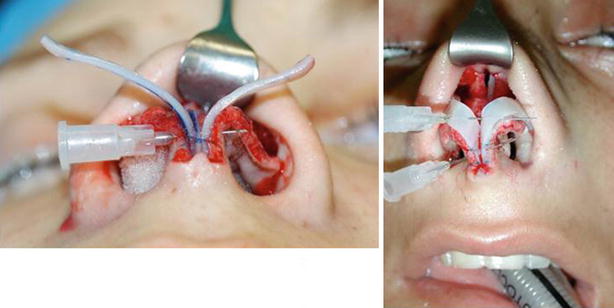


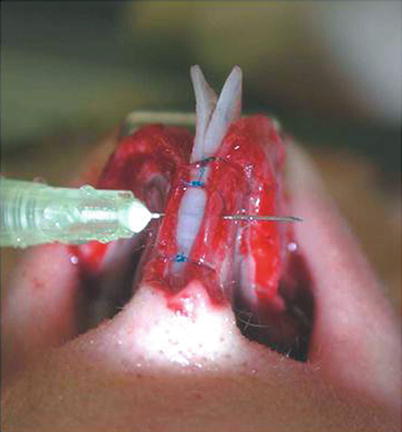
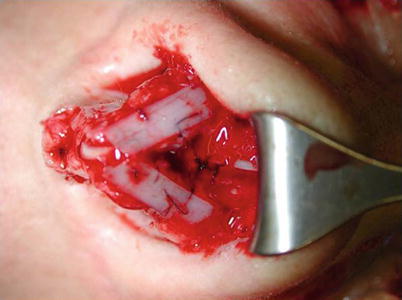
Fig. 12.1
Bending technique
Fig. 12.2
Scoring technique
Fig. 12.3
Dome division technique
Fig. 12.4
Split technique
Fig. 12.5
Batten graft technique
Fig. 12.6
(a, b) Supratip excision
12.2 Case Studies
12.2.1 Case 1: Suture and Shield Grafts
A 37-year-old female presented after previous septorhinoplasty with a 10-mm septal perforation, inadequate tip projection, and a persistent dorsal hump (Fig. 12.7). Using the open rhinoplasty approach and careful dissection at the ULC/dorsal septal junction, the septal perforation was repaired using the four-flap technique. Surgical exploration also revealed an unstructured mass of cartilage fragments within the nasal tip. The mass was divided vertically in the midline, and a double-layered (conchal) sandwich graft was then placed to stabilize and straighten the medial crura. After lowering the dorsum with a component technique, the overprojected upper lateral cartilages (ULCs) were invaginated and sutured to the dorsal septum as spreader flaps. The tip was then contoured by using horizontal mattress sutures to shape the scar-embedded cartilage fragments. A double-layered shield graft and bilateral alar rim grafts were then placed for better tip projection and tip contour, followed by a tip suspension suture to suspend and immobilize the tip complex.


Fig. 12.7
(a–b) Tip contouring with double-layered shield graft, horizontal mattress sutures, and bilateral alar rim grafts. (c–e) Front view, profile view, base view pre-op/post-op
12.2.2 Case 2: Alar Reconstruction with Septal Cartilage
A 26-year-old female presented for revision rhinoplasty complaining of an unattractive nasal profile (Fig. 12.8). Examination revealed facial asymmetry; a polly-beak deformity with a narrow, overprojected, and deviated dorsum; and pinching of the internal nasal valves. Using the external rhinoplasty approach, nasal exploration revealed heavy subcutaneous scarring and asymmetry of the lateral crura caused by overresection of the right crus and inadequate resection of the left. An overprojected and irregular dorsum was lowered to create a straight and smooth dorsal profile. Spreader flaps were then used to reconstitute the middle vault and eliminate internal valve collapse. The bony vault was also reshaped with bilateral osteotomies. Strips of autologous septal cartilage were then harvested to reconstruct the right intermediate and lateral crura, and transdomal sutures were used to contour the tip. Tip rotation was stabilized using a tip suspension suture with a posterior sling, and alar rim grafts were used for alar contour enhancement. The reconstructed tip complex was then covered with a double-layered allogenic fascia lata graft.

Fig. 12.8
(a) Overresected lateral crus right, inadequate trimming of the lateral crus left. (b) Reconstruction of the right overresected lateral crus by septal batten graft, then ala spanning sutures. (c–e) Front view, profile view, base view pre-op/post-op
12.2.3 Case 3: Fold-Under Flap Combined with Lateral Crural Overlay
A 25-year-old male presented for revision rhinoplasty (Fig. 12.9). Examination revealed a polly-beak profile deformity and external valve collapse during inspiration. On frontal view, the nose was canted to the patient’s right side, and on basal view an oblique columella resulted in nostril asymmetry. Using the external approach, the overprojected cartilaginous dorsum was lowered and reconstructed with spreader flaps. The tip was strengthened with fold-under flaps (lateral crural underlay technique) on both sides, and tip symmetry was achieved using a one-sided lateral crural overlap technique. The tip was further contoured using a shield graft harvested from the tragus, and alar rim grafts were placed bilaterally.

Fig. 12.9
(a–e) Tip reconstruction with fold-under flaps on both sides combined with an overlap technique on the left. Additional shield graft. (f–h) Front view, profile view, base view pre-op/post-op
12.2.4 Case 4: Combination Columellar Strut/Cephalic Fold-Under Flap/Suspension Suture with Anterior Sling
A 30-year-old female presented after unsuccessful rhinoplasty with nasal obstruction (Fig. 12.10). Examination revealed a deformed (oblique) anterior septum obstructing both nasal passages, and the right nostril was observed to collapse on gentle inspiration. The tip was bulbous, wide, and ptotic, with unusually thick skin and poor definition, and the dorsum was overprojected.
Using the open rhinoplasty approach, the residual septum was removed, and spreader grafts were used to create a straight neoseptum. After dorsal hump reduction and osteotomies, the neoseptum was replaced and sutured to the ULCs, nasal bones, and anterior nasal spine (ANS) using drill holes. Following columellar strut placement, the lateral crura were strengthened using cephalic fold-under flaps. A suspension suture with an anterior sling, combined with spanning sutures, was then used for tip rotation and contouring.


Fig. 12.10
(a–e) Extracorporeal septal reconstruction, cephalic fold-under flaps. (a) Severe septal deformity. (b) Extracorporeal septal reconstruction, cephalic fold-under flaps. (c–e) Front view, profile view, base view pre-op/post-op
12.2.5 Case 5: Technique: Supratip Excision
In cases of tip refinement with very thick and scarred tip skin, shrinkage and adherence of the skin envelope to the reduced cartilaginous framework is often incomplete and prone to dead space formation and additional subcutaneous scarring (Fig. 12.11). In order to achieve an attractive tip profile, there are only two options to eliminate this problem: either enlarge the framework to stretch the scarred and thickened tip skin or reduce the size of the nasal skin envelope. Since most patients will refuse a bigger nose to achieve better tip contour, reduction of the skin envelope may be advisable. To reduce skin volume and tighten the skin envelope, a supratip elliptical skin excision is performed in the midline just behind the tip-defining point. When the amount of skin excision is judged correctly, the wound edges collapse automatically and need almost no suturing. Only a subcutaneous suture approximation and supportive taping are required.


Fig. 12.11
(a) Scarred tip. (b) Contouring the tip with suture technique. (c) Non integrated shield graft to support the contouring. (d ) Supratip excision: technical details. (e–g) Polly-beak correction with supratip excision. Front view, profile view, base view pre-op/post-op
A 40-year-old female presented with a conspicuous polly-beak deformity after two previous rhinoplasties. The tip skin was extremely thick and sebaceous. The nostrils were also asymmetrical, and the endonasal examination revealed a septal deviation to the left and a subluxation of the caudal septum to the right. The right lateral crus also appeared to have been overresected.
Using an open rhinoplasty approach, the scars on the tip framework and the dorsum were removed, but the skin flap was not thinned. The caudal septum was then shortened at its base and sutured back to the ANS through transverse osseous drill holes. Harvesting of the left concha cartilage was challenging because of previous otoplasty, but it was still possible to fabricate a double-layered sandwich graft from the left ear. The graft was placed in the membranous septal pocket using a percutaneous columellar guiding suture and then sutured to the caudal septum as a septal extension graft. The weak lateral crura were then augmented with onlay batten grafts fashioned from ear cartilage on the left side and septal cartilage on the right. To improve tip contour, a nonintegrated shield graft was placed so that the graft projected slightly higher than the domes. As the final step, a longitudinal supratip skin excision was performed to eliminate the stubborn polly-beak deformity.
12.2.6 Case 6: Reconstruction of the Lower Framework with Septum via Bending Technique
A 27-year-old female presented drooped tip with overprojected dorsum after previous operation (Fig. 12.12). After opening the nose via external approach resection of both intermediate and both lateral crura has been revealed.
The septum was intact, so that after separating the ULC both upper and lower tunnels have been dissected, the dorsum was lowered then the central part of the septum has been harvested, leaving back a 25 mm wide framework. The bony pyramid was narrowed after low-to-low lateral, parasagittal medial, and transcutaneus transverse osteotomies. The excess of the ULC, which resulted from lowering the dorsal septum, was invaginated and fixed to the septum as spreader flaps. Two long strips from septal cartilage have been fixed to the residual medial crural, a columellar strut has been put in between the thin septal cartilage strips could be bended in the dome area, fixed by intradomal sutures and then the lateral part has been fixed directly to the scars on top of the vestibular skin. The contour was shaped by spanning suture, which has been fixed to the dorsal septum (tip suspension suture with posterior sling). A shield graft was placed and two layers of allogenic fascia covered the dorsum.


Fig. 12.12
(a–c) Reconstruction of the lower framework with bending technique using septal cartilage. (d–f) Front view, profile view, and base view preoperative and 17 months postoperative
12.2.7 Case 7: Reconstruction of the Lower Framework with Septum via Bending Technique
A 29-year-old female presented for revision rhinoplasty after two previous failed attempts at rhinoplasty elsewhere (Fig. 12.13). The patient sought correction of the C-shaped dorsal curvature, pinching of the dorsum, and poor tip projection. Using the open rhinoplasty approach, an S-shaped curvature of the dorsal septum was observed. Correction of the crooked L-strut involved shortening the caudal septum at its base so that it fit into the sagittal groove of the nasal spine, followed by suture fixation of the caudal septum. The cartilaginous dorsum was then lowered and reconstituted using spreader flaps to straighten and widen the middle vault. Strips of septal cartilage were then used to reconstruct the deformed nasal domes previously treated with vertical dome division. The newly created domes were then stabilized with a shield graft. Because of exceptionally thin nasal skin, the tip construct was also covered with two layers of allogenic fascia lata.


Fig. 12.13
(a–b) Reconstruction of the overresected LLCs with septal cartilage using bending technique. (c–e) Front view, profile view, base view pre-op/post-op
12.2.8 Case 8: Reconstruction of the Lower Framework with Septum via Bending Technique
A 24-year-old male presented for revision surgery after two previous rhinoplasties elsewhere (Fig. 12.14). He complained of a feminized nose with overresection of the dorsum, tip deformity, and alar retraction. Using the open approach, the tip framework was found to be severely damaged. Autologous septal cartilage was used to create narrow strips for tip reconstruction using the bending technique. Paired grafts were first sutured to the medial crura and then carefully thinned at the domes using a motorized drill equipped with a diamond fraise. This enabled folding of the grafts to create neodomes, which were then further contoured using transdomal sutures. The opposite ends were then sutured to the underlying lateral crura to contour the alar rims, and the domes were padded with a soft-tissue onlay. The dorsum was also augmented with conchal cartilage and covered with allogenic fascia lata.

Fig. 12.14
(a–c) Reconstruction of the overresected LLCs with septal cartilage using bending technique. (d–f) Front view, profile view, base view pre-op/post-op
12.2.9 Case 9: Reconstruction of the Lower Framework with Septum via Bending Technique
A 31-year-old female presented after two unsuccessful rhinoplasty procedures (Fig. 12.15). The patient complained of a persistent dorsal hump and a wide underprojected nasal tip. Open rhinoplasty revealed bilateral alar cartilage malformations involving the lateral and intermediate crura on both sides. Dorsal reduction was performed using the spreader flap technique to straighten and widen the dorsum, widen the internal valves, and improve the dorsal aesthetic lines. Thin battens of septal cartilage were used as onlay grafts to replace the nasal domes and to smooth the lateral crura. Tip sutures were then used to contour the domal replacement grafts and to conceal intermediate crural asymmetry. A well-defined and narrow tip with better projection was achieved.


Fig. 12.15
(a–c) Reconstruction of the overresected LLCs with septal cartilage using bending technique. (d–f) Front view, profile view, base view pre-op/post-op
12.2.10 Case 10: Reconstruction of the Lower Framework with Septum via Bending Technique
A 27-year-old female presented with fullness of the supratip after previous rhinoplasty (Fig. 12.16). The dorsum revealed irregularities, and she complained about deviation of the bony pyramid. Scars resulting from previous alar base resections were also quite obvious.
Surgical exploration using the open approach revealed total resection of both the lateral crura and the right intermediate crus. A large septal cartilage graft was harvested leaving a 15-mm L-strut. The nasal axis was straightened with osteotomies and placement of spreader grafts. The medial crural footpods were resected to narrow the columellar pedestal, and a columellar strut was placed for tip support. On the right side, the intermediate and lateral crura were reconstructed using a long cartilaginous strip fashioned from donor septal cartilage. The graft was thinned with a scalpel at the dome for easier bending. On the left side, a cartilage graft was fixed to the remnant intermediate crus and thinned at the dome; both domes were then formed using a transdomal suture. For better contour, a shield graft was sewn to the infratip, and because of thin nasal tip, skin allogenic fascia lata was used to cover the tip construct.


Fig. 12.16
(a–b) Reconstruction of the overresected LLCs with septal cartilage using bending technique, additional shield graft, covered with allogenic fascia. (c–e) Front view, profile view, base view pre-op/post-op
12.2.11 Case 11: Reconstruction of the Lower Framework with Septum via Bending Technique
A 29-year-old female presented after previous rhinoplasty with a wide and droopy nasal tip, pinched alae, a pseudo-hump deformity, and deviation of the nasal axis (Fig. 12.17).
Using the open approach, surgical exploration revealed previous resection of both lateral crura and a dislocated shield graft. A large piece of septal cartilage was harvested for graft fabrication while preserving a strong residual L-strut. After straightening and narrowing the bony pyramid with parasagittal medial osteotomies combined with percutaneous low-to-low lateral and transverse osteotomies, spreader grafts were placed for dorsal stabilization. The tip was also reconstructed using septal cartilage to create a double-layered columellar strut graft and lateral crural replacement grafts, which were sculpted with both transdomal and spanning sutures. A tragal graft was used to create a shield graft, which was covered with intercrural soft tissue. The original malpositioned shield graft was divided longitudinally and used to create bilateral rim grafts. To improve surface contour, the tip and dorsum were then draped in a layer of allogenic fascia lata.

Fig. 12.17
(a–d) Reconstruction of the overresected LLCs with septal cartilage using bending technique. (e–g) Front view, profile view, base view pre-op/post-op
12.2.12 Case 12: Reconstruction of the Lower Framework with Septum via Bending Technique
A 23-year-old female presented after two previous rhinoplasties with a slight nasal deviation resulting from a deformed dorsal septum in an asymmetric face (Fig. 12.18). Additionally, a conspicuous tip asymmetry with bossae formation was also observed. The sharp tip edges mimicked a poorly shaped tip graft protruding through the extremely thin nasal skin. Supratip fullness was also observed on profile examination.
Using an open surgical approach, exploration revealed severe overresection of both lateral crural cartilages. On the left side, the lateral crus must have been malpositioned because the remnants remained asymmetrical. Additionally, no reconstruction of the internal valve had been performed, and both valves were now exceedingly narrow. Treatment began by harvesting spreader grafts and two long thin cartilage strips for LLC reconstruction from the quadrangular septum. The paired tip grafts were then sutured to the medial crura, bent to create new domes, and secured with a transdomal suture. The lateral segments of the tip grafts were then sewn directly to the scarred vestibular skin to complete the LLC reconstruction. Final contouring of the reconstructed tip framework was achieved using spanning sutures in combination with a tip suspension suture with a posterior sling. To conceal the tip grafts, a layer of allogenic fascia lata was used to cover the reconstructed tip.
Straightening of the nasal axis was accomplished using paired spreader grafts to straighten the dorsal septum (and open the nasal valves), coupled with parasagittal medial and percutaneous low-to-low lateral and transverse osteotomies of the bony vault. Because of facial asymmetry, the axis of the nose could not be exactly vertical.
Fig. 12.18
(a–c) Different grafts from the septum: spreader grafts combined with reconstruction of the overresected LLCs using bending technique. (d–f) Front view, profile view, base view pre-op/post-op
12.2.13 Case 13: Reconstruction of the Lower Framework with Septum via Batten Graft Technique
A 31-year-old female presented after two prior cosmetic rhinoplasties with a conspicuous polly-beak deformity (Fig. 12.19). Surgical exploration with the open approach revealed complete absence of the right lateral crus and malpositioning of the intermediate crural remnant. Reconstruction included columellar strut placement followed by replacement of the missing right lateral crus with a batten graft fashioned from septal cartilage. A shield graft with carefully beveled edges was also placed to enhance tip contour and projection. Allogenic fascia lata was then used to camouflage the tip reconstruction.

Fig. 12.19
(a–c) Reconstruction of the overresected LLC using batten graft, columellar strut, and shield graft, covered with allogenic fascia lata. (d–e) Front view, profile view pre-op/post-op
12.2.14 Case 14: Reconstruction of the Lower Framework with Septum via Batten Graft Technique
A 39-year-old female presented 10 years after previous rhinoplasty (elsewhere) (Fig. 12.20). Examination revealed a wide, amorphous, and asymmetrical tip, bilateral alar retraction, and an inverted-V deformity of the middle vault. External rhinoplasty revealed total destruction of both lower lateral cartilages. Tip reconstruction was performed using a columellar strut and bilateral crural batten grafts fashioned from septal cartilage. Spanning sutures were then added for tip contouring, and spreader grafts were used to eliminate the inverted-V deformity. Finally, a cap graft fashioned from allogenic fascia lata was used to cushion the tip framework, and the dorsum was also camouflaged with a layer of allogenic fascia lata.


Fig. 12.20
(a–b) Reconstruction of the overresected LLCs using batten grafts and columellar strut. (c–e) Front view, profile view, base view pre-op/post-op
12.2.15 Case 15: Reconstruction of the Lower Framework with Septum via Batten Graft Technique
A 26-year-old male presented after unsuccessful rhinoplasty (elsewhere) (Fig. 12.21). The patient complained of a wide and droopy nasal tip. Open rhinoplasty revealed overresection of both lateral crura and missing portions of the left intermediate crus. In contrast, the cartilaginous dorsum showed no indication of previous surgical intervention. Septal cartilage replacement grafts were used to reconstruct the damaged nasal domes using a motorized drill to permit folding of the domes. After integration of the grafts into the residual tip cartilage, a shield graft was sutured to the infratip so that it extended above the reconstructed tip framework. This served to stretch the scarred and noncompliant tip skin for better tip definition. The dorsum was also lowered conservatively to create a straight dorsal profile.
Fig. 12.21
(a–d) Reconstruction of the overresected LLCs using batten grafts and shield graft. (e–g) Front view, profile view, base view pre-op/post-op
12.2.16 Case 16: Reconstruction of the Lower Framework with Septum via Batten Graft Technique
A 25-year-old female presented for revision rhinoplasty after treatment elsewhere (Fig. 12.22). Examination revealed a wide and amorphous tip, a polly-beak profile deformity, and a conspicuous inverted-V deformity. External rhinoplasty revealed prior resection of the lateral aspect of both lateral crura. Septal cartilage was used to create batten grafts to reconstruct the surgically weakened lateral crura. Spanning sutures were then used to contour the now rigid lateral crura. Tip projection was increased using a precisely shaped cap graft.