(1)
Klinik für Plastische Gesichtschirurgie, Marienhospital Stuttgart, Stuttgart, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-662-49706-7_11) contains supplementary material, which is available to authorized users.
Keywords
Tip contourTip rotationTip projectionTip positionTip volumeTip definitionTip width11.1 Surgical Principles
Alterations of nasal tip contour are perhaps the most challenging aspect of cosmetic rhinoplasty. And because tip contour must harmonize with the surrounding facial features in a natural but pleasing manner, some degree of surgical tip refinement is a goal of nearly every cosmetic rhinoplasty. However, in addition to constituting a major determinant of facial beauty, the tip is also an integral component of the human nasal airway. Hence, surgical alterations to the nasal tip framework must be circumspect in order to prevent impairment of nasal airway function. Naturally weak tip cartilages are at increased risk of collapse with surgical manipulation, and cartilage size may not always correspond to cartilage strength.
In addition to surgical technique, various architectural and biomechanical properties govern the outcome of tip rhinoplasty. Rollin K. Daniel differentiates between the three intrinsic factors of volume, definition, and width and the three extrinsic factors of position, rotation, and projection—all critical determinants of tip aesthetics. Yet, from an analytical and utilitarian standpoint, the characteristics of contour, rotation, and projection are perhaps the most useful.
Although surgical changes in contour, rotation, and projection of the nasal tip framework are prerequisites for a satisfactory cosmetic transformation, architectural changes can be profoundly altered by the characteristics of the overlying skin/soft-tissue envelope. Noses with ultrathick tip skin have greater bulk, weight, and volume (Fig. 11.1), which can obscure skeletal definition, promote unwanted tip ptosis, and resist tip narrowing. On the other hand, mild to moderate deformities of the underlying tip framework can be diminished or even totally concealed by thick nasal skin. Conversely, ultrathin nasal skin offers better surface definition, less bulk, and greater ease of tip narrowing, but thin skin provides little or no camouflage of underlying skeletal imperfections, and shrink-wrap contracture is typically more severe in thin-skinned noses. And although surgical changes to the skeletal framework are still paramount, the prudent surgeon will recognize the limitations of unfavorable skin types and counsel patients accordingly.
In addition to the impact of the overlying skin/soft-tissue envelope on tip aesthetics, changes in the surrounding nasal anatomy may also have an impact on nasal tip aesthetics. Since the nose represents a complex three-dimensional structure, surgical changes in one area may have a secondary anatomic and/or visual impact on another. For example, reducing dorsal height gives the illusion of nasal lengthening, and a slight increase in tip rotation may be needed to offset this phenomenon. Conversely, augmentation of a low radix may create the illusion of a counterrotated tip owing to cephalic repositioning of the nasal starting point. Since the final cosmetic outcome is determined by the impact of direct skeletal alterations coupled with influences of both the skin envelope and illusory changes, the combined impact of these factors must be carefully considered during preoperative planning and analysis.

Fig. 11.1
Debulking of the tip
11.1.1 Nasal Tip Contour
Nasal tip contour depends mainly on the three intrinsic factors of volume, definition, and width. The surgical options available to change tip contour include excisional techniques, suture techniques, or combined techniques. Because excisional techniques are irreversible and destructive, they have become increasingly less popular. Alternatively, suture techniques that are potentially reversible and conserve intrinsic skeletal support are quickly becoming the workhorse of contemporary rhinoplasty.
The goal of tip refinement surgery is a slender and attractive lobule while avoiding an overly pointed, “uni-tip” deformity. In most noses, this requires two distinct cartilaginous domes separated anteriorly by a small amount of soft tissue to create a gentle rounding of the most projecting tip segment as seen from the basal view. Domal width can be reduced with “intradomal” or “dome-unit” mattress sutures to narrow domal angulation. However, care must be taken to avoid overtightening of the suture, which can lead to collapse of the lateral crus and lobular pinching. Similarly, “transdomal” mattress sutures can be used to bring individual domes into closer proximity and to improve domal symmetry, but care must be taken to place the suture posteriorly so as to allow a slight divergence of the domes anteriorly (Fig. 11.2), thereby preventing unsightly pinching of the infratip lobule. Divergence of the domal folds can also be established using a shield graft to maintain a slight flaring of the intermediate crura (Fig. 11.3). In many instances, the use of transdomal sutures may obviate the need for intradomal tip sutures, since domal narrowing often occurs as the domes are sutured in closer proximity. In some cases, excessive subcutaneous soft tissue can obscure tip definition to the point that surgical debulking of the subcutaneous soft tissues is necessary for optimal surface contour enhancement of the tip (Fig. 11.1). Although volume reduction can be accomplished with trimming of the cephalic margin, cephalic resection should be performed judiciously because overresection of the lateral crura is one of the most common causes of postsurgical tip deformity. The cephalic resection should be performed medial to the junction of the intermediate and lateral crus to prevent collapse and/or retraction of the lateral segment. Conservative resection is advised in all cases, but particularly with weak tip cartilages. Following resection, weak lateral crura should be stabilized using ancillary techniques such as onlay batten grafts, lateral crural strut grafts, or fold-under flaps. The last one is our preferred technique (Fig. 11.4). However, exceptionally thick and stiff cartilage necessitates a combination of excisional and suture techniques (Fig. 11.5), since suture techniques alone are seldom adequate.
Tip definition is defined by Rollin K. Daniel as the visibility or distinctive setting apart from the dome defining point from the rest of the ala. Tip definition can be enhanced using tip suture techniques to sculpt the tip cartilages or by placing a shield graft to increase tip projection (Fig. 11.3). Good tip definition is always a goal of tip rhinoplasty. However, aesthetic preferences vary, and we strive to create a more or less straight alar margin between the tip lobule and the lateral ala as seen on basal view (Fig. 11.6). Alar rim grafts, placed into skin pockets dissected along the nostril rims via the marginal incision (Fig. 11.7), are used liberally to prevent notching of the nostril rim (the so-called seagull deformity) and/or retraction of the alar rim. When the need for alar rim grafts becomes evident after skin closure, we insert the graft via an external skin incision placed within the alar crease (Fig. 11.6). Graft length is variable, but when necessary, the graft may extend all the way into the soft-tissue triangle to prevent deformation of the entire alar rim (Fig. 11.7).
To correct excessive tip volume and bulbosity, conservative resection of the lateral crus at the cephalic margin is a standard part of our refinement technique. However, we perform the traditional cephalic resection only in thick crural cartilages. In thin or medium-thickness cartilage, we retain the cephalic margin as a fold-under flap to flatten and strengthen the lateral crus (Fig. 11.4). This is done by first dissecting the vestibular skin off the undersurface of the lateral crus and then incising the cephalic segment from above. The excised segment is then folded under as an underlayment graft such that the concave surfaces are placed face-to-face. The fold-under graft is then sutured with 6-0 PDS sutures. Alternatively, to correct concavity of the lateral crus, we suture the cephalic margin as a fold-over flap to bend the lateral crus in the opposite direction (Fig. 11.8). In both cases, the retained cephalic margin serves to correct contour deformities while simultaneously strengthening the lateral crus against collapse. In this manner, we can later apply spanning sutures to control flaring without fear of deforming the lateral crura.
Another method for strengthening the lateral crus is horizontal mattress sutures (Fig. 11.9). Using horizontal mattress sutures to flatten the lateral crus simultaneously serves to increase crural rigidity to allow placement of spanning sutures with less risk of crural deformity (Fig. 11.10).
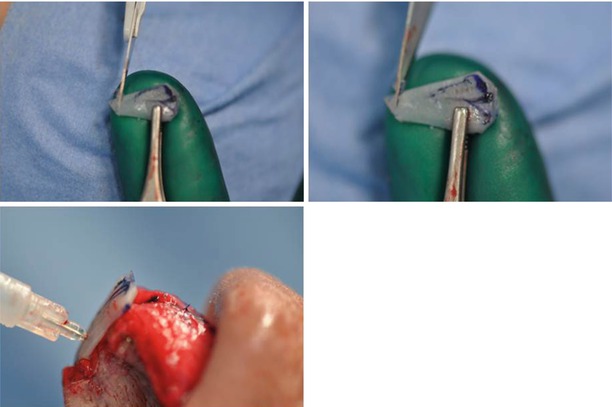
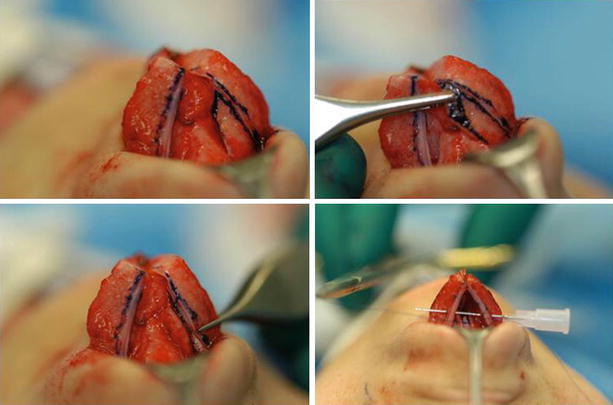
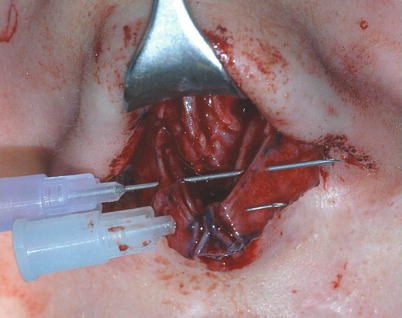
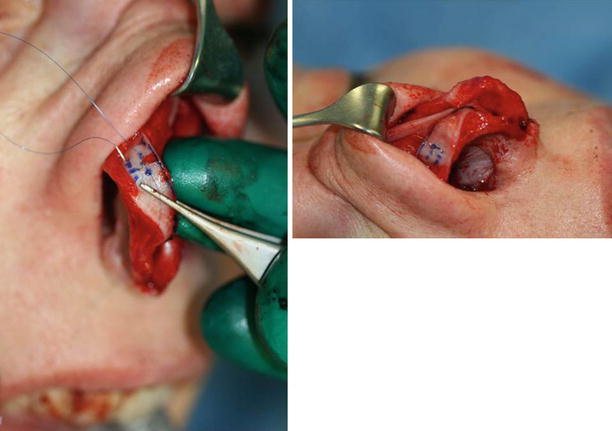
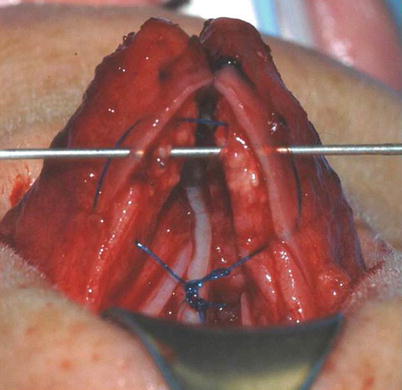
Fig. 11.2
(a, b) Suture technique, preparing the transdomal suture
Fig. 11.3
Shield graft
Fig. 11.4
Combined suture/cutting technique fold-under flap technique (lateral crural underlay)
Fig. 11.5
Preparing ala spannning sutures
Fig. 11.6
(a, b) Rim grafts
Fig. 11.7
(a, b) Rim grafts
Fig. 11.8
(a–c) Lateral crural overlay technique
Fig. 11.9
Horizontal mattress suture
Fig. 11.10
Spanning sutures combined with tip suspension suture and posterior sling
11.1.2 Projection of the Tip
Tip projection is an important parameter defined as the distance the nose protrudes from the face. Abnormalities in tip projection include both overprojection and underprojection. Typically in the overprojected tip, the patient complains about a big nose. However, when analyzing a large nose, it is important to differentiate between an overprojected dorsum (nasal hump), an overprojected tip (Pinocchio nose), or both an overprojected dorsum and an overprojected tip (rhinomegaly). In cases of rhinomegaly where the overprojected tip is not recognized and treated appropriately, even after a successful dorsal realignment the nose will appear to “jump off the face” because of the persistent and now even more obvious overprojected nasal tip. Although an isolated overprojected tip is easily recognized, a normally projected tip with an adjacent saddle-nose collapse may also give the (false) impression of an overprojected tip. Therefore, care must also be taken to differentiate between these two similar looking but distinctly different contour deformities.
Early techniques for treatment of the overprojected tip relied upon segmental excision of the nasal domes without suture reapproximation of the alar cartilages to restore skeletal continuity. The result was often tip ptosis and polly-beak formation and/or a pinched tip. However, safer and more effective alternatives, such as the sliding techniques, are now available. A variety of sliding techniques have been described, including alar dome reduction (Hamra), alar cartilage overlap (Adamson), lateral crural overlap (Kridel/Foda), or alar cartilage setback (Foda). All of these techniques rely upon altering the relative length of the medial and lateral crura, and sliding techniques can be used both medially (Fig. 11.11) and laterally (Fig. 11.12). Medial sliding techniques decrease tip projection while simultaneously decreasing tip rotation (tip counterrotation). In contrast, lateral sliding techniques decrease tip projection while simultaneously increasing tip rotation. By performing both medial and lateral sliding techniques simultaneously, opposing changes in tip rotation can be offset to prevent changes in tip rotation if desired. Alternatively, the balance can also be manipulated to achieve subtle changes in tip rotation and/or tip alignment when necessary. The overall impact of adjusting medial or lateral crural length can be easily understood using the “tripod” model of tip dynamics as originally described by Anderson.
Medial sliding techniques are also indicated for correcting deformities involving the junction of the medial and intermediate crura. Often a medial sliding technique is indicated for correction of asymmetrical buckling at the junction of the medial and intermediate crus, but counterrotation is contraindicated. In this scenario, the buckled cartilage is divided, and the cartilages are overlapped to eliminate the buckling. However, to eliminate counterrotation, the upper segment is rotated cephalically, creating a partial overlap and a protruding upper segment that must be excised (Fig. 11.13).
Another means of achieving tip deprojection is the push-down technique (Fig. 11.14). The push-down technique involves repositioning the medial crura inferiorly in closer proximity to the premaxilla. This works best in noses with a protruding caudal septum, since the medial crura can be sutured to the caudal septum for fixation. Depending upon the natural length of the medial crura, the push-down technique can dramatically reduce tip projection without transecting the tip cartilages. As adjunct to tip deprojection, excess skin can be excised from the columella (Fig. 11.15). Typically, this is performed at the transcolumellar incision in order to avoid an additional scar.
A variety of techniques are also available for increasing tip projection. In the wide tip, a small amount of increased tip projection is achieved simply with intradomal suture placement (Fig. 11.16). Columellar strut placement will increase tip projection per se only minimally, but it does serve to stabilize weak and underprojected tip cartilages. And for many techniques that increase tip projection, a columellar strut is essential. One such technique is the lateral crural steal procedure. This technique recruits cartilage from the lateral crus to elongate the medial crus and thus to increase tip projection. This is accomplished by folding the lateral crus at a point lateral to the existing nasal dome in order to create a new, more projected nasal dome (Fig. 11.17). However, a columellar strut or equivalent graft is needed to strengthen the medial crura and support the newly projected domes.
Other means of increasing tip projection are augmentation grafts such as cap grafts (Fig. 11.18), onlay grafts (Fig. 11.19), or even a nonintegrated shield graft (Fig. 11.3). However, these grafts are all associated with the potential risk of graft visibility from gradual thinning and/or contracture of the overlying skin. Moreover, unsightly graft prominence can develop many years following graft placement. Consequently, in noses with thin or intermediate skin thickness that are at risk for excessive graft visibility, we use a soft-tissue overlay graft such as allogenic fascia lata or perichondrium to cover the cartilage framework and prevent excessive graft prominence (Fig. 11.19). Finally, in cases where tip projection is exceedingly poor, such as some ethnic noses, total reconstruction of the nasal tip framework may be needed to achieve adequate tip projection (Fig. 11.20).
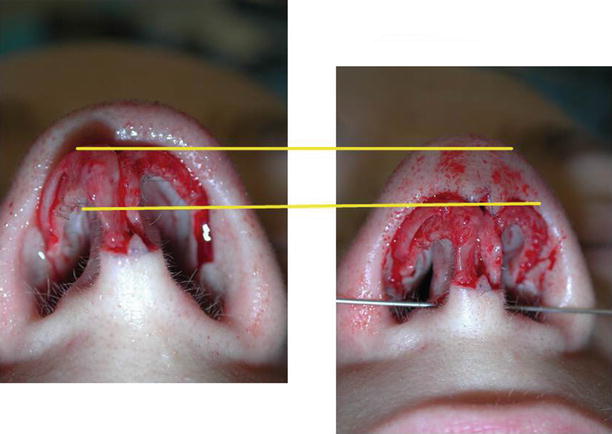

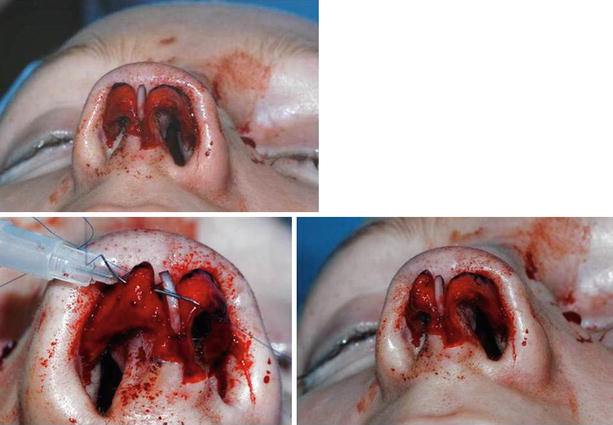
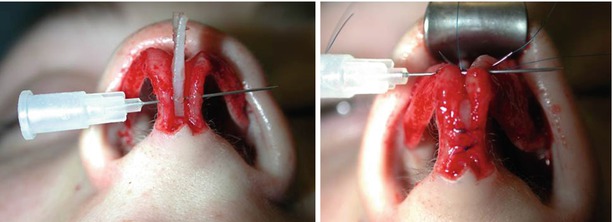

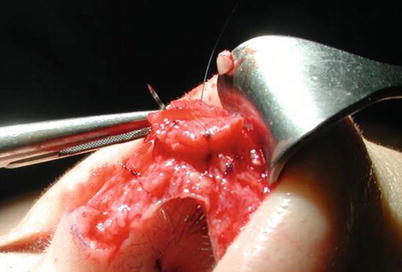
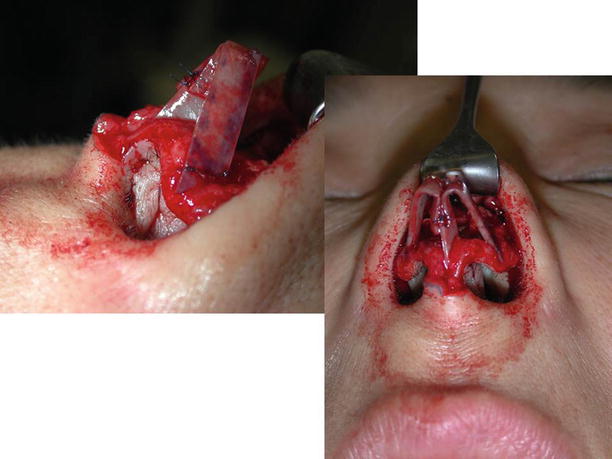
Fig. 11.11
(a, b) Medial sliding technique
Fig. 11.12
(a–d) Lateral sliding technique
Fig. 11.13
(a, b) Medial sliding with cranial rotation
Fig. 11.14
Push down
Fig. 11.15
Shortening of the columella
Fig. 11.16
Intradomal sutures (identical with dome defining suture (RK Daniel))
Fig. 11.17
Lateral crural steal technique
Fig. 11.18
Cap graft from cartilage
Fig. 11.19
Cap graft from fascia
Fig. 11.20
Reconstruction of a new lower framework from strips of septal cartilage, fixed to a columellar strut from the septum
11.1.3 Rotation of the Tip
The extent of tip rotation governs the absolute length of the nose. According to Jack Gunter, nasal length is defined as the distance separating the nasal starting point from the tip defining point. Positioning of the nasal starting point can be altered by either raising or lowering radix height. Increasing radix height by augmenting the nasion will result in cephalic repositioning of the nasal starting point, whereas lowering the nasion will deproject the radix and shift the nasal starting point caudally. Although repositioning the nasal starting point is cosmetically significant, these changes are primarily visual, since the absolute distance from the nasal tip to the brow ridge does not change. However, unlike changes in radix height, which fail to alter absolute nasal length, changes in tip rotation physically alter absolute nasal length. For instance, when tip rotation is increased, the lobule is repositioned cephalically and absolute nasal length is decreased. Conversely, when the nasal tip is counterrotated (i.e., reduced tip rotation), the lobule moves away from the nasal starting point, and absolute nasal length is increased. For this reason, changes in tip rotation can be used to correct an overly long or short nose. The overly short and upturned “piggy” nose is highly objectionable because it results in excessive nostril show, whereas the overly long nose is often characterized by a droopy and aged appearance. Because tip rotation is largely governed by tip support, a droopy nasal tip may also be associated with an acute nasolabial angle, which is often an indicator of inadequate tip support.
One of the most difficult challenges in rhinoplasty is nasal lengthening. Even in primary rhinoplasty, it is usually far more difficult to lengthen the nose than to shorten it, since the soft-tissue envelope and scar contracture often resist substantial nasal elongation. Previously we used the closed rhinoplasty approach in conjunction with a complete transfixion incision to lengthen the nose. However, this approach typically cut all tip support mechanisms, resulting not only in counterrotation of the tip but also in tip deprojection and ultimately in tip ptosis. While this approach can be used for modest nasal lengthening, the procedure is imprecise and unpredictable. Moreover, using finger pressure applied to the nasolabial angle to predict the drooping of the tip and the extent of nasal lengthening is equally unreliable and will only provide a crude estimate of counterrotation. Finally, weakening of septal support may also lead to some degree of tip counterrotation. However, trimming the anterior septum is both destructive and imprecise and is ill-advised. On the other hand, using the medial crural sliding overlay technique will produce noticeable counterrotation, but at the expense of tip deprojection. Consequently, this approach for nasal lengthening should be reserved for short, overprojected noses (Fig. 11.21).
At present we prefer the external rhinoplasty approach for nasal lengthening, and cartilage augmentation grafts are our preferred method for creating precise increases in nasal length. For modest increases in nasal length, a shield graft, or several layers of shield graft, can be used to counterrotate the tip and create modest increases in nasal length (Fig. 11.22). However, for sizable increases in nasal length, the most effective technique in our hands is to lengthen the entire cartilaginous framework. One approach for aggressive lengthening is to place an ultrawide columellar strut graft in which the upper half is much broader than the typical columellar strut graft. The best graft for this purpose is the double-layered conchal sandwich graft (Fig. 11.23). Owing to the extra graft width and double-layered graft construction, the conchal sandwich graft can be positioned and secured to the caudal septum using a tongue-in-groove fixation. In addition to providing a strong and stable union, tongue-in-groove fixation to the caudal septum serves to buttress the elongated tip against upward displacement by a tight or inelastic skin envelope. For noses that require even greater elongation, we use extended spreader grafts to maintain positioning of a columellar strut graft (Fig. 11.24). Alternatively, septal cartilage can be used to create a septal extension graft for aggressive nasal elongation (Fig. 11.25). There are two different ways to fix such a graft: end to end or side to side. Using an end-to-end fixation, the septal extension graft must be contoured carefully so that it fits precisely with the anterior septal border. To provide a strong fixation to the septum, we prefer using either a splinting graft of perpendicular ethmoid bone or extended spreader grafts for tip stabilization. Alternatively, a side-to-side fixation is possible, which gives a firmer construction, but by overlapping cartilages, a slight asymmetry may result.
In contrast to nasal lengthening, decreasing nasal length is not restricted by soft-tissue elasticity. Modest decreases in nasal length can be achieved by increasing tip rotation. Historically this has been accomplished with excision of the cephalic margin of the lateral crus—the so-called “cephalic trim” procedure. Although this technique simultaneously reduces tip volume and potentially facilitates cephalic tip rotation, it also frequently results in unsightly upward retraction of the alar rims. Because of that possible complication, the cephalic trim should be regarded as an unreliable and unpredictable technique for tip rotation. Shortening the nose by excising a vertical strip of vestibular skin or nasal mucosa and trimming the caudal septum are other destructive procedures that should be reserved for extreme circumstances in which severe tissue excess justifies potentially irreversible tissue excision.
Our preference for modest reductions in nasal length is to rotate the nasal tip using suspension sutures. In noses with cartilage of sufficient rigidity, we often combine the suspension suture with a spanning suture to prevent the lateral crural flaring that results from aggressive tip rotation (Fig. 11.10). However, with weak tip cartilages, the combined suture may result in concave collapse of the lateral crura. Consequently, in noses with weak tip cartilage, the lateral crura must first be strengthened with cephalic fold-under (Fig. 11.4) or fold-over flaps (Fig. 11.8) or with augmentation grafts such as crural batten grafts. When using the combined suture, a spanning suture is placed first and then knotted to preserve the desired tip contour. The same suture is then sewn to the dorsal septum, tightened to achieve the appropriate degree of tip rotation, and knotted a second time to suspend the tip (7 see Fig. 11.10).
When pure tip rotation is desired without changes in lateral crural contour, we use nonresorbable 4-0 monofilament suspension sutures without the combined spanning suture. Two suspension options are available: suspension with a posterior sling (Fig. 11.26) or suspension with an anterior sling (Fig. 11.27). Although the posterior sling utilizes a deeply buried and fully hidden knot, the anterior sling offers easier insertion and greater precision with an increased risk of a visible subcutaneous knot.
For this purpose, R.K. Daniel uses a suture catching the posterior part of the medial crura and fixing them to the anterior border of the septum (called a tip position suture).
Fixation of the medial crura to the anterior septal border by the tongue-in-groove technique is also very effective to control tip rotation. This technique requires a long septum. Therefore, we always try to avoid shortening the anterior septum in case we want to apply this technique for a precise tip rotation. The disadvantage of the tongue-in-groove technique is the loss of natural mobility. Therefore, some patients complain about unnatural stiffness, which is a high but acceptable price to be sure that the tip does not droop (Fig. 11.28).
If the anterior border of the septum is far behind so that such a tongue-in-groove technique would lead to an overrotated tip, the following technique advised by Tim Marten is possible: the anterior border of the septum is cut but stays pedicled to the periosteum of the premaxilla. Then this strip of cartilage is down-rotated until the medial crura can be fixed to it in the planned way. To fix this amount of rotation, the new position of this anterior septal border is anchored by extended spreader grafts. Alternatively, a thin splint from the perpendicular plate is also possible for fixation.
Specifically in older patients in whom an excess of skin exists that will not shrink after cranial rotation and may lead to additional wrinkles, a nose lift (Fig. 11.29) at the root of the nose will not only remove the excess of skin but will also be an additional technique for cranial rotation of the tip, especially if the undermined skin envelope of the nose is fixed to the frontal periosteum.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


