(1)
Department of Pharmaceutics and Drug Delivery, The University of Mississippi, Oxford, MS 38677, USA
(2)
Institute for Drug Delivery and Biomedical Research, Bangalore, India
Keywords
Skin electroporationFentanylInsulinCo-enhancement techniquesMicrodialysisNoninvasive samplingNeedle-type electrodesIntradermal vaccinationElectrogene transfer and safety of needle-type electrodes8.1 Introduction
Rapid expansion of the field of biotechnology yielded a vast number of clinically significant peptides, proteins, and other gene-based therapeutic agents. A sharp inclination in transition toward the discovery and development of aforementioned biological agents has been observed in the recent past, owing to better cure rates and relatively lesser side effects in treating complex diseases. However, administration of such biomolecules had been highly challenging and often invasive in nature. Classic examples are administration of insulin and vaccines, where an alternative to needle-free delivery is highly desired. Transdermal delivery route offers remarkable advantages over conventional routes in terms of better patient compliance, programmable drug delivery, and avoidance of drug destruction in the liver and/or gut. However, only a handful of therapeutic agents with a combination of optimum distinctive features permeated well across the skin’s structural barrier, stratum corneum. Transdermal electroporation was pursued as an active technique to reversibly compromise this barrier functionality of the skin, thus increasing the range of therapeutic agents that was delivered across it. Electroporation technique was demonstrated in the early 1970s, and its major application was confined to transfection of mammalian cells with DNA for gene therapy. This technique was adapted in transdermal drug delivery research recently due to its capability of delivering molecules across human skin. In electroporation, short-lived moderate to high-voltage pulses are applied on the skin to generate temporary aqueous pathways in the lipid microstructures present in the stratum corneum.
The scope of this chapter is to give an insight to the readers about various therapeutic applications of skin electroporation technique with a concise review of the research literature.
8.2 Safety and Tolerability of Skin Electroporation
The major criteria for clinical inception of novel drug delivery platforms center around its safety, efficacy, and tolerability. When these goals are met, it is likely that the drug delivery technology would achieve better commercial success, high level of patient acceptance, and compliance therefore. Electroporation technique had been thoroughly investigated in the past for its potential therapeutic applications and significant safety and tolerance limits.
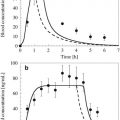
Following electrical treatment, the electrical resistance of the stratum corneum decreases drastically within a range of μs and was found to be associated with various changes in skin biophysical parameters (Dujardin et al. 2002; Pliquett et al. 1995). Electroporation-induced structural changes in human skin were investigated using differential scanning calorimeter, X-ray diffraction technique, and freeze-fracture electron microscopy. Results from these analyses confirmed perturbations induced in the lipid structural assembly in the stratum corneum which was primarily responsible for the drop in electrical resistance (Jadoul et al. 1997, 1998, 1999). Skin impedance, in in vivo testing in rats, decreased by more than fivefolds following ten pulses of 1000 V for 100 μs duration, and normal values were regained 6 h after the electroporation was finished (Fig. 8.1). However, pulsing with ten pulses of 350 V for 5 ms duration took a little longer than 6 h to return to pre-pulsing values. A combination of chromametry, transepidermal water loss (TEWL) measurements (Fig. 8.2), and laser Doppler flowmetry was employed to assess relevant biophysical changes induced in the skin. The measurement of TEWL values indicated a significant rise followed by highest enhancements observed at 7 min post-pulsing (for both 350 V and 1000 V) and baseline regained after 35 min (Fig. 8.3). From Fig. 8.4, it was evident that no significant injury, cell death, and tissue necrosis were produced in the skin following both the pulsing protocols (350 V and 1000 V) (Dujardin et al. 2001, 2002).
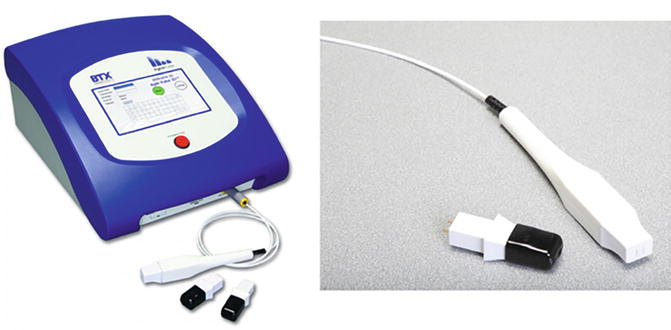
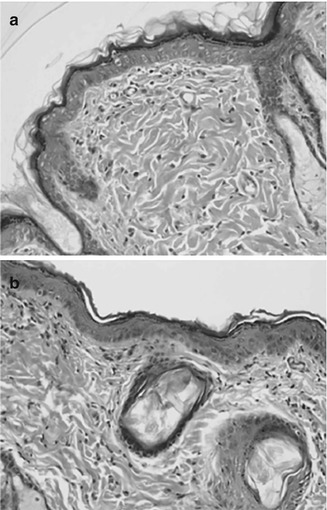
Fig. 8.1
Relative impedance value following pulsing protocols, 10× (350 V for 10 ms), 10x (1000 V for 100 μs); n = 6 (Reproduced from Dujardin et al. 2002, 222. With kind permission from Elsevier Inc., USA)
Fig. 8.2
TEWL (g/m2 h) after skin electrical treatment at the cathode, anode, and control sites; n = 6 (Reproduced from Dujardin et al. 2002, 223. With kind permission from Elsevier Inc., USA)
Fig. 8.3
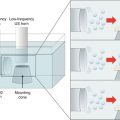
Agile pulse in vivo system from BTX® Instrument Division, Harvard Apparatus Inc., USA, for intradermal vaccine and gene therapy (Reproduced with kind permission from Harvard Apparatus Inc., USA)
Fig. 8.4
Hematoxylin and eosin stained slides of (a) control skin and (b) electroporated skin 4 days after pulsing with 10× (1000 V for 100 μs). No occurrence of inflammation or tissue necroses was detected following electroporation treatment (Reproduced from Dujardin et al. 2002, 226. With kind permission from Elsevier Inc., USA)
From a study in pig model, the tolerability of electroporation pulses was assessed in relation to iontophoresis technique (Riviere et al. 1995). In the test group, exponentially decaying pulses of magnitude 0, 250, 500, and 1000 V were applied followed by iontophoresis treatment with 0, 0.2, 2.0, and 10 mA/cm2. In the control group, similar electrical pulses were applied but without the post-pulsing iontophoresis treatment. An evaluation was performed on the skin reactions produced in both groups for comparison. In Table 8.1, the first set of data for each voltage corresponds to the skin reactions induced 5 min after combined pulsing and iontophoresis application. The second set of data was collected in a similar fashion after 4 h. Although, the occurrence of erythema was observed to increase with the pulse voltage, the skin reactions were mostly due to iontophoresis application and not electroporation. In the control group, erythema, edema, and petechiae were not observed following the electroporation treatment alone (not shown in table).
Table 8.1
Gross observations of the skin under the active electrode after electroporation treatment of pig skin at different pulse voltages followed by iontophoresis
Pulse | Erythema | Edema | Petechiae | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
(V) | 0.0 | 0.2 | 2.0 | 10.0 | 0.0 | 0.2 | 2.0 | 10.0 | 0.0 | 0.2 | 2.0 | 10.0 | ||
(Current, mA/cm2) | (Current, mA/cm2) | (Current, mA/cm2) | ||||||||||||
0 | 0.00 | 1.75 | 1.25 | 1.75 | 0.00 | 1.75 | 1.25 | 1.75 | 0.00 | 0.75 | 0.75 | 1.50 | ||
0.00 | 0.50 | 0.50 | 0.50 | 0.00 | 1.00 | 1.00 | 1.50 | 0.00 | 0.00 | 0.00 | 0.50 | |||
250 | 0.00 | 0.75 | 1.25 | 2.00 | 0.00 | 0.75 | 1.50 | 1.67 | 0.00 | 0.00 | 0.50 | 1.67 | ||
N/A | 0.00 | 0.50 | 0.00 | N/A | 0.50 | 1.00 | 1.00 | N/A | 0.00 | 0.50 | 1.00 | |||
500 | 1.00 | 1.25 | 1.75 | 2.30 | 0.00 | 1.00 | 1.50 | 1.33 | 0.00 | 0.00 | 0.00 | 0.00 | ||
N/A | 0.00 | 0.50 | 0.00 | N/A | 1.50 | 1.00 | 1.00 | N/A | 0.00 | 0.00 | 0.00 | |||
1000 | 2.60 | 1.25 | 1.50 | 2.00 | 0.80 | 1.25 | 1.00 | 1.75 | 0.00 | 0.00 | 0.25 | 1.50 | ||
1.67 | 1.00 | 0.00 | 1.00 | 0.67 | 0.50 | 1.00 | 1.00 | 0.00 | 0.00 | 0.50 | 0.50 | |||
In a clinical study involving electrochemotherapy treatment for malignant melanoma, a pulse protocol comprising eight pulses of 1.3 kV/cm2 for 100 μs was applied directly onto the tumors on the skin surface, in human subjects. Patients reported instantaneous contractions in the muscle site lying in the vicinity of the site of electroporation application. This effect was attributed to the direct electrical excitation of nerves, by the current applied to the skin (Byrne et al. 2005). However, it was regarded as clinically harmless, and it was concluded that the application of high-voltage pulses was very well tolerated. Thus, electroporation was found to be safe for administration in human subjects, similar to iontophoresis.
8.3 Design Considerations for Electroporation Device and Electrode Systems for Transdermal Applications
The advancement of skin electroporation from preclinical phase to clinical development and eventual routine medical practice mandate the development of robust pulse generators and applicator electrodes for electroporation administration (Rabussay 2008). The primary focus of the design considerations include establishment of clinical safety for regulatory approval and patient acceptability. Also, design of a compact pulse generator and applicator, which is simple and usable by the patients, would avoid frequent clinical visits. A list of general key variables that should be considered during optimization of the design of the electroporation device is described in Table 8.2. The scope of this section hence provides a brief description about the pulse generator, the choice of electrode systems available for transdermal and intradermal drug delivery, and the functional approach toward the electrode systems design.
Table 8.2
Design space for electroporation generator and applicator – key variables
Component | Variables |
|---|---|
Generator | |
Individual pulse protocol | Voltage |
Pulse length | |
Polarity | |
Waveform | |
Multiple pulse protocol | Variables of individual pulse protocols |
Number of pulses | |
Frequency [Hz] | |
Electrode polarity change pattern | |
Applicator | |
Field strength (V/cm) | Distance between electrodes at application site |
Field homogeneity | Electrode shape |
Field orientation | Electrode shape and relative position to application site |
Current density and resistance | Effective electrode surface area |
Handle | |
Safe and ergonomic design | |
Efficient application |
The pulse generator is the primary source of electrical current and can generate either square-wave or exponential decay wave patterns, based on the intended clinical applications. The pulse generators are tunable to produce electrical currents of various intensity, pulsatile mode, polarity, and duration of time that perfectly suits the varied clinical needs and nature of treatment.
A commercially available electroporation device ECM® 830 (from BTX® Instrument Division, Harvard Apparatus Inc., USA) (Fig. 8.5) which works in conjunction with Tweezertrode and caliper electrode systems (Fig. 8.6) is currently used for various in vitro and in vivo applications. The tip of the electrodes is usually made of metal and/or alloy like stainless steel, brass, and platinum with an effective surface area ranging from 0.7 to 2 cm2. For major applications involving intradermal vaccine delivery, a modified pulse generator, as the one shown below (Fig. 8.3), was developed which works in conjunction with the minimally invasive needle-type electrodes (MIE). A MIE is inserted into the skin for electropulsing following intradermal administration of the vaccines. An example to this is a 4 × 4 array of needle-type electrodes made of trocar-gold (depicted below in Fig. 8.7) developed for intradermal administration of vaccines (Broderick et al. 2011). Also, Inovio® Pharmaceuticals Inc., USA, had developed needle-type electrodes that possess dual functionality of an injector and an applicator electrode. Generally, extra precaution should be taken while choosing the conducting material and designing the array of needle-type electrodes.
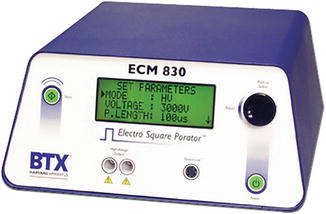
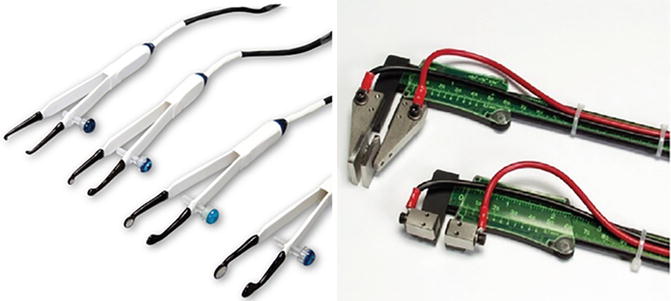

Fig. 8.5
ECM® 830 Electro Square Porator™ from BTX® Instrument Division, Harvard Apparatus Inc., USA (Reproduced with kind permission from Harvard Apparatus Inc., USA)
Fig. 8.6
Tweezertrodes and caliper electrodes from BTX® Instrument Division, Harvard Apparatus Inc., USA (Reproduced with kind permission from Harvard Apparatus Inc., USA)
Fig. 8.7
A prototype development of minimally invasive 4 × 4 array trocar-gold-coated electrodes for intradermal applications (Inovio® Pharmaceuticals, USA) (Reproduced from Broderick et al. 2011, 261. With kind permission from Nature America Inc., USA)
A needle-free microelectrode array was fabricated and demonstrated for painless administration of transdermal electroporation. The influence of different electrode design parameters on level of pain induction was evaluated in human subjects (parameters: size and skin contact surface area of electrode and distance between individual electrodes). Two electropulsing protocols, at the threshold of transdermal electroporation [60 pulses at 150 V for 1 ms (pulse interval, 0.1 and 1 s)], were applied on human forearm using cylinder-type electrodes of varying diameter. Under identical pulse protocols, electrodes with a larger skin contact surface area were less tolerable than the smaller contact surface area electrode (Fig. 8.8). For the electrodes of same size, the pain score increased with the distance between individual electrodes (Fig. 8.9). Based on these findings, an array with 11 × 11 microelectrodes made of copper (0.36 mm2 skin contact area) was fabricated for painless electroporation administration in humans. The distance between adjacent electrode pads within the microarray was fixed at 0.6 mm (Fig. 8.10). In addition, the pain scores reported by human subjects during electropulsing with microelectrode array and commercially available Red DotTM electrodes (3M Health Care, St. Paul, MN, USA) were compared. Results indicated that single pulse administration at 120 V–0.2 ms using Red DotTM electrodes produced a pain score ~10 against negligible pain score reported for 60 pulses administration at 150 V–0.2 ms using microelectrode array (Fig. 8.11).
Fig. 8.8
 Iontophoresis: Basic Principles
Iontophoresis: Basic Principles
 Microporation in Penetration Enhancement
Microporation in Penetration Enhancement
 Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
 Gene Transfer to the Skin by Physical Methods of Delivery
Gene Transfer to the Skin by Physical Methods of Delivery
 Magnetophoresis: Skin Penetration Enhancement by a Magnetic Field
Magnetophoresis: Skin Penetration Enhancement by a Magnetic Field
 Combined Use of Iontophoresis and Other Physical Methods
Combined Use of Iontophoresis and Other Physical Methods




Effect of the diameter of the individual electrode on pain sensation in human subjects following electroporation with 60 pulses at 150 V–0.2 ms. Black bar represents pulse interval of 0.1 s and gray bar represents pulse interval of 1.0 s. The smaller the diameter of the electrode (less skin contact area), the lesser the pain elicited (Reproduced from Wong et al. 2006, 559. With kind permission from Elsevier Inc., USA)
Related posts:
Microporation in Penetration Enhancement
Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
Gene Transfer to the Skin by Physical Methods of Delivery
Magnetophoresis: Skin Penetration Enhancement by a Magnetic Field
Combined Use of Iontophoresis and Other Physical Methods
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
