(22.1)
Viable skin
where C is the drug concentration, D is the diffusion coefficient, h is the thickness of the stratum corneum, H is the thickness of the skin, t is time, and k is the first-order enzymatic reaction rate. The subscripts sc and vs stand for stratum corneum and viable skin, respectively. We can solve the diffusion phenomena through skin using Eqs. (22.1) and (22.2) to obtain the following initial and boundary conditions:
(22.2)
Initial condition

Boundary conditions


 where C d is the concentration in the drug formulation, K sc is the partition coefficient between the skin surface and the drug formulation, and K sc/vs is the partition coefficient between the stratum corneum and the viable skin.
where C d is the concentration in the drug formulation, K sc is the partition coefficient between the skin surface and the drug formulation, and K sc/vs is the partition coefficient between the stratum corneum and the viable skin.
We simplify the skin penetration as a single-layered skin model because the skin penetration flux of drugs is controlled by the stratum corneum’s barrier function. Under the conditions of steady-state penetration with perfect sink condition, Eq. (22.1) can be replaced by the following equation:
where Q is the cumulative amount of drug and ∆C is the concentration gradient between both ends of the skin.
(22.3)
22.3 Physical Enhancement
In the past two decades, the progress in biotechnology and bioinformatics has led to novel and potent drugs (i.e., peptides, antibodies, oligonucleotides, and small interfering RNAs (siRNAs)) and the possibility to establish safer and more effective drug delivery strategies. Transdermal delivery would be advantageous for these new drugs because they are metabolized easily in the gastrointestinal tract by oral delivery. However, these drugs can hardly penetrate through the skin because of their high molecular weight and hydrophilic properties. Because the skin penetration flux is simplified as Eq. (22.3), the flux is increased by the improvement of D sc, ∆C, K sc, and h individually and at the same time. Three effective enhancement methods are (1) to increase the diffusion coefficient in the stratum corneum, (2) to increase the concentration in the drug formulation and in the stratum corneum, and (3) to decrease the thickness of the stratum corneum or to create new pathways across the stratum corneum. The physical enhancements are achieved by the use of external energy to add a driving force for the skin penetration and mechanical force to reduce the barrier function of the stratum corneum.
22.3.1 Iontophoresis
Iontophoresis using a low current density (the limitation is ≤ 0.5 mA/cm2 for human skin) is a superior method for the percutaneous absorption of drugs with a molecular weight between 200 and 300 Da (Yoshida and Roberts 1992). This enhancement method is based on electrorepulsion and/or electroosmosis. Electroosmosis is a convective flow that goes across the stratum corneum from the anode to the cathode when the pH value of the skin surface is more than 4.0 (Kim et al. 1993). Thus, the flux of nonionized drugs is also increased by electroosmosis. The diffusion equation with no enzymatic reaction across the stratum corneum under iontophoresis becomes the following:

where z is the charge number of the ionized drug, F is the Faraday constant, E is the electric field, R is the gas constant, T is the absolute temperature, and u is the velocity of the convective flow.
(22.4)
Because the electrorepulsion and electroosmosis occur only under an electric field and are affected by the current density, it becomes possible to achieve a continuous, pulsed, and reversed delivery of drugs, to terminate the application immediately, and to reduce inter- and intraindividual variation. The advantages of iontophoresis bring possibilities for transdermal therapeutic systems. Iontophoresis has been studied for systematic and topical delivery, and some devices using electric fields such as the E-TRANS® (Alza/Ortho-McNeil Pharmaceutical Co.) for fentanyl (Gupta et al. 1999), the LidoSite® (Vyteris Inc.) for lidocaine (Pasero 2006), the IontoPatch® (Travanti Pharma Inc.) for dexamethasone (Chaturvedula et al. 2005), and the GlucoWatch® (Cygnus Inc.) as a glucose monitor (Garg et al. 1999) have actually come onto the market.
It must be noted that there are several reports in which iontophoresis caused irreversible damages to the skin (Burnette and Ongpipattanakul 1988; Inada et al. 1994; Wang et al. 1993). Miyagi et al. (2006) reported about the effect of molecular weight of drugs on the iontophoretic enhancement of flux. The flux of vitamin B12 (MW = 1355) increased appreciably in parallel with the constant current density (~0.6 mA/cm2) and reached a plateau after the current was turned off (Fig. 22.1). In contrast, the flux of fluorescein isothiocyanate (FITC)-dextran (FD-4, average MW = 4400; FD-10, average MW = 11,000; FD-20, average MW = 19,000) increased continuously after a lag time (0.5 h for FD-4 and 1.5 h for FD-10 and FD-20) (Fig. 22.2). Kanikkannan (2002) also reported that iontophoresis might not be a suitable method for the transdermal delivery of peptides (>7000 Da). These results indicate that iontophoresis might be able to enhance the flux of drugs with high molecular weight (≥5 kDa), but it is impossible to control the flux.
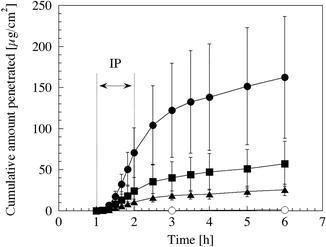
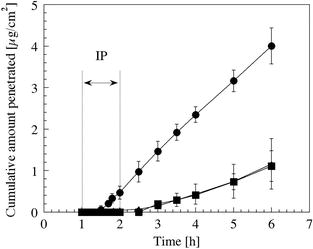
Fig. 22.1
Effect of current density on the skin penetration of vitamin B12. The electric field was applied for 1 h after 1 h of passive transport. Closed circles, 0.6 mA/cm2; closed squares, 0.3 mA/cm2; closed triangles, 0.15 mA/cm2; open circles, control experiment (0 mA/cm2). IP iontophoresis (Reproduced with permission from The Society of Chemical Engineers, Japan)
Fig. 22.2
Effect of iontophoresis (0.3 mA/cm2 for 1 h) on the flux of FITC-dextran (circles, FD-4; triangles, FD-10; squares, FD-20) (Reproduced with permission from The Society of Chemical Engineers, Japan)
22.3.2 Electroporation
Electroporation is also electro-assisted enhancement methods as well as iontophoresis and was originally used as a transfection method entering deoxyribonucleic acid (DNA) into the cell; high-voltage pulse applications for very short durations of time make transient pores in the cell membrane (Zerbib et al. 1985). Prausnitz et al. (1993) first reported the use of electroporation in transdermal delivery research. They achieved the enhancement of the transdermal flux of calcein (MW = 623, −4 charge) at in vitro and in vivo experiments. After this report, the skin penetration enhancement for macromolecules has been reported (Lombry et al. 2000; Riviere et al. 1995; Vanbever et al. 1998; Zhang et al. 2002; Zhao et al. 2006). Electrical studies have shown that the enhancement mechanism of electroporation and the factors of voltage, pulse length, and pulse rate affect the drug penetration flux (Banga et al. 1999; Denet et al. 2004; Sharma et al. 2000; Vanbever et al. 1996). Skin resistance dramatically decreases on a time scale of milliseconds by high-voltage pulses (Prausnitz 1996). The fast decrease of skin resistance causes the creation and expansion of pores in the stratum corneum (Pliquett et al. 1995), and the slow decrease may involve the change of the stratum corneum structure by thermal effects (Pliquett and Gusbeth 2000). The pathways created by electrical pulse immediately close after cutting off the pulse, and, however, the skin resistance does not completely recover when electrical stimulus was too strong (Pliquett et al. 1995). Riviere et al. (1995) observed skin irritation after application of electroporation (a single exponential voltage pulse for 5 ms, ≤ 1000 V). An electroporation pulse had a transient erythema and no adverse irritation. Therefore, the advantages of electroporation are: (1) to cause insignificant skin damage, (2) to show the enhancement effect quickly, and (3) to increase the skin flux of macromolecules with a molecular weight greater than 7000 Da which limit for iontophoresis (Denet et al. 2004; Kanikkannan 2002).
22.3.3 Ultrasound
The enhancement of drug penetration is determined by ultrasound parameters (i.e., frequency, intensity, duty cycle, and duration of application) (Shirouzu et al. 2008). This is because physicochemical phenomena, rising temperature, acoustic streaming, the generation of convective flow, and the cavitation (Barnett et al. 1994; Liu et al. 1998; Mitragotri et al. 2000) caused by sonophoresis are influenced by: each ultrasound parameter, skin models, physicochemical properties of drugs, and experimental conditions. The flux of lidocaine hydrochloride (MW = 270, Fig. 22.3a) and that of vitamin B12 (Fig. 22.3b) were influenced by the ultrasound frequency (2 MHz and 300 kHz, 410 J/cm2). The vitamin B12 flux was also affected by the energy flux (intensity × treatment time × duty cycle) (Fig. 22.4) (Shirouzu et al. 2008). The enhancement mechanism involves mechanical, thermal, and physiological changes of the skin, in particular the imploding cavitation bubbles that disrupt the structure of the lipid bilayers in the stratum corneum (Tezel and Mitragotri 2003).
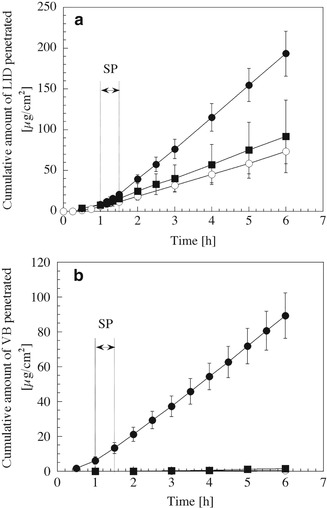
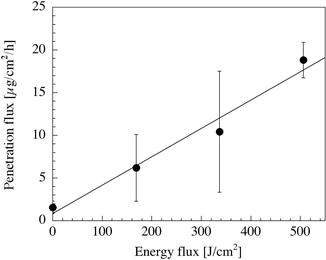
Fig. 22.3
Enhancement of the skin penetration of lidocaine hydrochloride (LID, (a)) and vitamin B12 (VB, (b)) by sonophoresis (SP) for 30 min. The energy flux of ultrasound was controlled at 410 J/cm2. Closed circles, low-frequency ultrasound (300 kHz); closed squares, therapeutic-frequency ultrasound (2 MHz); open circles, control experiment without sonophoresis
Fig. 22.4
Influence of energy flux (intensity × treatment time × duty cycle) of ultrasound on the penetration flux of vitamin B12. The ultrasound frequency was 300 kHz. The flux increased in proportion to energy flux (Reproduced with permission from The Society of Chemical Engineers, Japan)
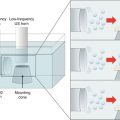
Sonophoresis is divided into three categories based on frequency: low-frequency (~kHz), therapeutic-frequency (1–3 MHz), and high-frequency (3–16 MHz) ultrasound. Bommannan et al. (1992) reported that high-frequency ultrasound increased the flux of salicylic acid and, at the same time, resulted in the structural alteration of skin tissue by the application of heat for 20 min. Therapeutic-frequency ultrasound is widely used in treatment, diagnosis, and physiotherapy. Therapeutic-frequency ultrasound at the intensity within 0–2 W/cm2 can induce reversible changes in the skin barrier and can enhance the flux of low molecular weight drugs (Mitragotri et al. 1995; Yamashita et al. 1996). However, it hardly improves the flux of high molecular weight drugs. The sonic waves of low-frequency ultrasound can deeply penetrate into the skin tissue, and, moreover, low-frequency ultrasound generates cavitation bubbles at lower intensity than therapeutic-frequency ultrasound. Low-frequency sonophoresis (20 kHz, 7 W/cm2, 50 % duty cycle) is used for the enhancement of high molecular weight drugs, insulin (MW = 5805 Da), heparin (12 k–15 kDa), and interferon-gamma (IFN-γ) (15 k–25 kDa) (Mitragotri et al. 1996; Mitragotri and Kost 2001). The US Food and Drug Administration (FDA) recently approved the SonoPrep® system (55 kHz, 15 W/cm2, Santra Medical Co.) as a transdermal delivery system for lidocaine. This system, using low-frequency ultrasound, is expected to be used as a needle-free blood glucose monitor.
Sonophoresis is an excellent method for transdermal drug delivery, but some researchers have reported skin tissue damage caused by sonophoresis under the higher intensity. Low-frequency ultrasound (20 kHz) at intensities lower than 2.5 W/cm2 did not affect skin tissues, whereas intensities of 5.2 W/cm2 caused irreversible changes in skin tissue (Boucaud et al. 2001). The skin is a water-rich tissue, and, thus, enzyme deactivation may certainly occur in the skin tissue by cavitation. The effect of the intensity and duration of ultrasound application (1 MHz, 4.3 W/cm2) on the bioconversion of an ester drug was investigated using a hairless mouse skin in vitro (Fig. 22.5) (Hikima et al. 1998). Enzyme deactivation may be partly responsible for free radicals generated in the reservoir solution and tissue fluid during an ultrasound pretreatment of the skin. More research is needed to identify the interactions among ultrasound parameters and to establish the safe use of drugs for transdermal therapeutic systems.
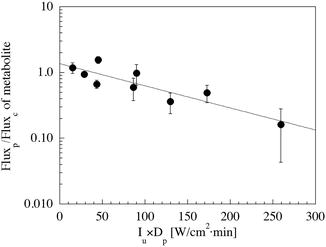
Fig. 22.5
Ratio of the flux of metabolite in skin treated by ultrasound (Fluxp) to the flux of metabolite in untreated skin (the control experiment, Fluxc) as a function of the product of intensity (I u) and treatment time (D p) (Reproduced with permission from Springer)
22.3.4 Microneedles
Microfabrication technology for drug delivery has been used in oral delivery (Verma et al. 2000), dermal delivery (Prausnitz et al. 2003), and implantable delivery (LaVan et al. 2003; Staples et al. 2006). Microneedles have been fabricated using microelectromechanical systems (MEMS) and have been developed to enhance the flux without the pain of piercing, as microneedles do not reach the nerve endings at the upper dermis. The drug application by microneedles was classified according to the material and design: (1) solid microneedles made from silicon, metal, and polymer that pierce the stratum corneum before drug application (Martanto et al. 2004; Hikima et al. 2012), (2) solid microneedles from metal and polymer coated with drug (Gill and Prausnitz 2007), (3) solid microneedles from biodegradable polymer coated with drug and contained the drug (Park et al. 2006), and (4) hollow microneedles from metal and polymer for drug solutions (Häfeli et al. 2009).
The Macroflux® transdermal microprojection delivery system with titanium microneedles coated with drug and the microstructured transdermal system (MTS) microneedle patch were developed by ALZA Co. and 3 M, respectively. Intracutaneous immunization with Macroflux® had similar immunoglobulin G (IgG) titers compared to intramuscular, subcutaneous, and intradermal injections (Matriano et al. 2002). Low-dose influenza vaccines with NanoPass® comprised of hollow silicon microneedles resulted in immunogenic reactions similar to the full-dose intramuscular vaccination (Damme et al. 2009). Microneedles may be suitable for the intracutaneous delivery of high molecular weight drugs, but there have been some reports that the insertion depth of a microneedle into the stratum corneum is influenced by the shape of the microneedle (Bal et al. 2010), the force of insertion (Davis et al. 2004), and the skin compaction during microneedle insertion (Martanto et al. 2006). Therefore, further detailed investigations into the mechanisms of drug transport by microneedles through the stratum corneum and the mechanical properties of the stratum corneum are necessary.
22.4 Combination of Iontophoresis with Other Physical Enhancement Methods
Chemical and physical enhancers have been studied for their use with transdermal therapeutic systems, to achieve active transport and to control the penetration flux of drugs. However, researchers reported that the strength of an undesirable stimulus, dermatitis, and irreversible skin damage increases in proportion to the enhancement effect of enhancers on the penetration flux of drugs (Boucaud et al. 2001; Ledger 1992). Thus, the application of enhancers in humans is limited due to their undesirable side effects. Protein and peptide drugs with high molecular weights do not penetrate across the skin easily (Kanikkannan 2002), and the penetration flux continuously increases after the electric current is removed (Miyagi et al. 2006). Therefore, researchers have been investigating the combined use of enhancers for reasons of safety, economy, and efficacy (Fang et al. 2002; Mitragotri 2000; Wang et al. 2005). Moreover, the combination of enhancers leads to the synergistic enhancement of transdermal drug delivery. There are many reports about the synergistic enhancement by the combined use of enhancers, such as the combinations of iontophoresis with chemical enhancers (Pillai et al. 2004; Rastogi and Singh 2005), iontophoresis with electroporation (Chang et al. 2000), iontophoresis with sonophoresis (Fang et al. 2002; Le et al. 2000; Shirouzu et al. 2008), iontophoresis with microneedles (Katikaneni et al. 2009; Lin et al. 2001), as well as sonophoresis with chemical enhancers (Johnson et al. 1996; Lavon et al. 2005), sonophoresis with electroporation (Kost et al. 1996), laser radiation with microdermabrasion (Fang et al. 2004), and others.
However, some researchers reported also a lower penetration flux when a combination of enhancers was used compared to the use of a single enhancement method. Denet et al. (2003) indicated that the electroosmotic flux during iontophoresis (0.25 mA/cm2 for 3 h or 0.5 mA/cm2 for 9 h) was decreased by the accumulation of a positively charged drug, timolol maleate, in the stratum corneum by electroporation pretreatment (400 V, 10 msec, 10 pulses). Singh and Jayaswal (2008) reported that the chemical enhancer Azone® inhibited the effect of an electric current (0.45 mA/cm2, 6 h) on 5-FU transport because it interacted with the components of the stratum corneum. X-ray, attenuated total reflectance Fourier transform infrared spectroscopy (ATR-FTIR), and differential scanning calorimetry (DSC) studies revealed that the pretreatment with the chemical enhancer hexadecyltrimethylammonium bromide changed the electrical and structural properties of the stratum corneum, with the result that the skin penetration flux of propranolol hydrochloride decreased (Chesnoy et al. 1999). Therefore, the mechanisms underlying the penetration enhancement by each enhancer must be further investigated so that the appropriate combination of enhancers can be identified.
22.4.1 Combination of Iontophoresis and Electroporation
While iontophoresis directly acts on the drug molecule and the movement of water through the stratum corneum, electroporation causes the change of stratum corneum structure. These methods have a different penetration mechanism, thereby the combined use of iontophoresis and electroporation could synergistically enhance the skin penetration flux of drug. Examples of the combined use of iontophoresis and electroporation are summarized in Table 22.1. Although electrical pulses of lower voltage less than 100 V followed by iontophoresis did not increase the flux of salmon calcitonin (MW = 3600), the flux was enhanced synergistically by the combined use of iontophoresis and electric pulse of 120 V (Chang et al. 2000). Ching et al. (2012) studied whether three different molecular weight biomarkers, urea (MW = 60 Da), osteopontin (MW = 33 kDa), and prostate-specific antigen (MW = 34 kDa), can be extracted from the skin by the combination of iontophoresis and electroporation in vitro. This technique is well known as reverse iontophoresis that is used as a diagnostic method by extracting molecules through the skin (Garg et al. 1999; Mize et al. 1997). Ching et al. (2012) concluded that transdermal extraction of prostate-specific antigen and osteopontin was possible only when applying reverse iontophoresis in combination with a high-voltage (≥ 296 V/cm) electroporation.
Table 22.1
Examples of the combined use of iontophoresis and electroporation
Drugs/chemicals | Applied conditions | Skin | Ref. |
|---|---|---|---|
Luteinizing hormone-releasing hormone | EP: 1 pulse of 1000 V IP: 0.5 mA/cm2, 30 min | Human, in vitro | Bommannan et al. (1994) |
Salmon calcitonin | EP: 6 pulses of 60, 100, and 120 V, 10 ms each IP: 0.5 mA/cm2, 4 h | Human, in vitro | Chang et al. (2000) |
Buprenorphine HCl | EP: 20 pulses of 500 V, 10 ms IP: 0.5 mA/cm2, 4 h | Human and pig, in vitro | Bose et al (2001) |
Dextran sulfate | EP: 6 pulses of 100, 250, and 500 V, 10 ms IP: 0.5 mA/cm2, 6 h | Human and pig, in vitro | Badkar and Banga (2002) |
Human parathyroid hormone (1–34) | EP: 100, 200 and 300 V, 20 pulses of 100 ms pulse length with 1 s interval between each pulse IP: 0.2 mA/cm2, 12 h | Porcine, in vitro | Medi and Singh (2003) |
Insulin | EP: 10 pulses of 150 or 300 V, 10 ms IP: 0.4 mA/cm2, 1 h | Rat, in vivo | Tokumoto et al. (2006) |
Ferric pyrophosphate | EP: 100 pulses of 120 V, 10 ms at 5 Hz IP: constant voltage (0.5, 2, 4 V), 30 min | Porcine, in vitro | Vaka et al. (2011) |
Urea, prostate-specific antigen, osteopontin | EP: 10 pulses/s of 74, 148, 296, and 592 V/cm, 1 ms IP: 0.3 mA/cm2 | Porcine, in vitro | Ching et al. (2012) |
Iontophoresis can control the skin penetration flux of drugs by switching current on/off, and, on the other hand, electroporation can enhance the flux of macromolecules. The combined use of iontophoresis and electroporation may be possible to control the flux of macromolecules; however, it may be difficult for resealing pathways created by electrical pulse immediately. Therefore, further detailed investigations are needed for the practical application of the combined use of iontophoresis and electroporation.
22.4.2 Combination of Iontophoresis and Sonophoresis
The combined use of iontophoresis and sonophoresis is a practical approach to enhance the flux synergistically, because the electric properties of skin tissue are not affected by ultrasound treatment at all. Table 22.2 summarizes the literature regarding the combined use of iontophoresis and sonophoresis. The frequency of the ultrasound was an important factor for the synergistic enhancement. The skin was pretreated by ultrasound (300 kHz and 2 MHz) for 30 min, and then electric field (0.35 mA/cm2, 1 h) was applied to the skin (Fig. 22.6). The combination of therapeutic-frequency ultrasound and electric field did not cause the synergistic enhancement of vitamin B12. Hikima et al. (2009) reported the effect of the application time of sonophoresis (Fig. 22.7). The flux of vitamin B12 increased to 48 times compared to the control flux when 30 min ultrasound and 1 h iontophoresis were applied simultaneously. On the other hand, a 177-fold synergistic enhancement of the drug flux was achieved when the electric field applied after the ultrasound pretreatment. These results may indicate that sonophoresis changes the stratum corneum structure by cavitation and iontophoresis produced the additional forces of electroosmosis.
Table 22.2
 Iontophoresis: Basic Principles
Iontophoresis: Basic Principles
 Microporation in Penetration Enhancement
Microporation in Penetration Enhancement
 Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
 Gene Transfer to the Skin by Physical Methods of Delivery
Gene Transfer to the Skin by Physical Methods of Delivery
 Magnetophoresis: Skin Penetration Enhancement by a Magnetic Field
Magnetophoresis: Skin Penetration Enhancement by a Magnetic Field
 Therapeutic Applications of Electroporation
Therapeutic Applications of Electroporation




The combined use of iontophoresis and sonophoresis
Related posts:
Microporation in Penetration Enhancement
Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
Gene Transfer to the Skin by Physical Methods of Delivery
Magnetophoresis: Skin Penetration Enhancement by a Magnetic Field
Therapeutic Applications of Electroporation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
