CHAPTER 8 The SMAS facelift – restoring facial shape in facelifting
Introduction
The works of Skoog, Mitz and Peyronie enlightened plastic surgeons to the possibility of repositioning descended facial fat to the anatomic position of youth, providing an alternative to skin envelope tightening to enhance contour in the aging face. The recognition that sub-SMAS dissection offered a technical solution for facial rejuvenation spawned multiple anatomic studies to delineate an accurate understanding of facial soft tissue anatomy. This led to further investigations which more clearly defined both the anatomic and morphologic changes which occur in the aging face, leading to a plethora of technical approaches for facial rejuvenation. In reviewing the literature, good results can be seen utilizing what appears to be very different technical approaches. In reality, most of these seemingly different technical procedures share a common theme that contour restoration is predominantly through the re-elevation of facial fat as opposed to skin envelope tightening. While good results are possible through a variety of techniques, in my opinion, all methods have advantages, disadvantages and limitations, with the ultimate result often dependent upon underlying skeletal support and the quality of facial soft tissues for a particular patient. From my perspective, the key to consistent results in facelifting is not the particular technique utilized, but rather the preoperative aesthetic analysis and how the operative plan is individualized according to the aesthetic needs of the patient.
Physical evaluation – patient planning
• Skin quality and elasticity.
• Subcutaneous fat accumulation.
• Contour change developing from attenuation of deep layer support, i.e. jowling, deep nasolabial fold; and platysma banding with cervical obliquity.
• Degree of skeletal support – malar prominence, mandibular ramus height and length of mandibular body.
• The relationship between malar convexity and submalar concavity.
Anatomic considerations
1. Although there is variation in the thickness of the various layers from patient to patient, structures within each layer are anatomically constant. On a two-dimensional basis, the facial nerve exhibits a variety of branching patterns, but on a three-dimensional basis, the facial nerve always lies within a specific anatomic plane. This anatomic arrangement allows the surgeon to perform extensive sub-SMAS dissection safely, as long as the dissection proceeds at a level superficial to the plane of the facial nerve.
2. There is significant variability in terms of the thickness of the superficial fascial layer (SMAS). This variability of SMAS thickness is obvious from patient to patient. Also, the thickness of the SMAS will vary from one region of the face to another. Overlying the parotid gland, within the temporal region (temporoparietal fascia) and within the scalp (galea), the superficial fascia (SMAS) represents a substantial, discrete layer. As the superficial fascia is traced anteriorly in the face, overlying the masseter, buccal fat pad, and into the malar region, the SMAS tends to become thinner and less substantial. To elevate the superficial fascia in these areas requires precise dissection, so that the flap is thick enough to be useful in facial contouring.
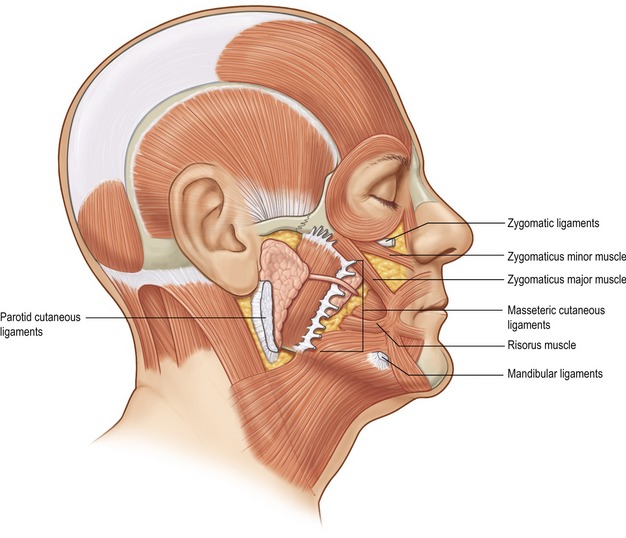
3. The muscles of facial expression are arranged in four anatomic layers which overlap one another. The muscles that are encountered in facelifting, including the platysma, orbicularis oculi, zygomaticus major and minor, and risorius muscle, are all superficially situated mimetic muscles. This is in contrast to deeply situated mimetic muscles such as the buccinator and mentalis muscle. Most of the muscles of facial expression lie superficial to the plane of the facial nerve. Because these muscles are superficial to the plane of the facial nerve, they receive their innervation along their deep surfaces. The only muscles within the facial soft tissue architecture that lie deep to the plane of the facial nerve are the mentalis, buccinator, and levator anguli oris muscles. Because these muscles lie deep to the plane of facial nerve, they receive their innervation along their superficial surfaces.
4. The muscles of facial expression, which are situated superficially within the facial soft tissue architecture and are involved with the movement of facial skin, are invested by the superficial fascia, which lines both the superficial and deep surfaces of these muscles. Because these muscles are invested by superficial fascia, this SMAS-mimetic muscle complex forms a single anatomic and functional unit whose components work together to move facial skin during animation.
5. Deep to the SMAS-mimetic muscle complex lies the deep facial fascia. The deep facial fascia represents a continuation of the superficial layer of the deep cervical fascia cephalad into the face. Where this fascial layer is identified, it is given specific nomenclature. Overlying the parotid gland, the deep fascia is termed “parotid fascia” or “parotid capsule”; overlying the masseter muscle, it is termed “masseteric fascia”; and in the temporal region, it has been termed “deep temporal fascia.” The significance of the deep facial fascia is that all the facial nerve branches within the cheek lie deep to the deep facial fascia. Typically, these nerve branches course deep to the deep fascia until they reach the muscles of facial expression that they innervate, at which point they penetrate the deep fascia to innervate these mimetic muscles along their deep surfaces (Fig. 8.1).
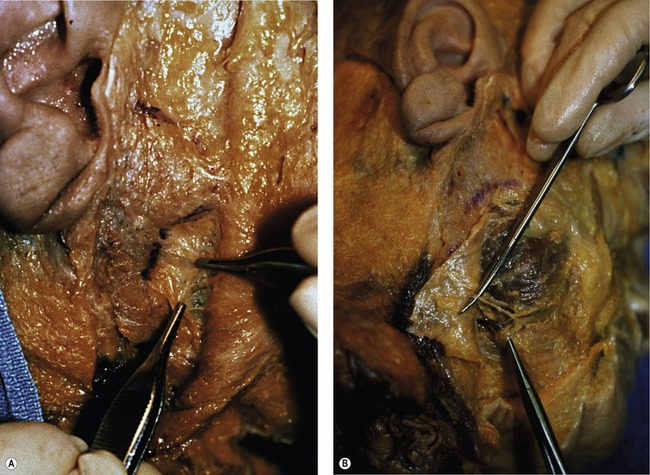
In an overview of the architectural arrangement of the facial soft tissue, the essential point to grasp is that there is a superficial component of the facial soft tissue that is defined by the superficial facial fascia and includes the SMAS and those anatomic components that move facial skin (including superficially situated mimetic muscle invested by SMAS, the subcutaneous fat, and skin). This is in contrast to the deeper component of the facial soft tissue, which is defined by the deep facial fascia and those structures related to the deep fascia (including the relatively fixed structures of the face, such as the parotid gland, masseter muscle, periosteum of the facial bones, and facial nerve branches) (Fig. 8.2). As the human face ages, many of the stigmata that are typically seen in aging relate to a change in the anatomic relationship that occurs between the superficial and deep facial fascia.