The Midface Lift
Kenneth D. Steinsapir
Samantha M. Steinsapir
EDITOR COMMENTARY
This chapter provides a variety of techniques for midface lifting from use of alloplastic implants to sub- and preperiosteal lifts by periorbital, temporal scalp, and oral gingival approaches.
In the past 15 years, oculofacial surgeons have been grappling with what is essentially a new frontier in the field: midface surgery. In contrast to many of the classic techniques of oculoplastic surgery, midface surgery is still in a process of rapid evolution and flux, with insufficient peer-reviewed literature to adequately assist the surgeon who is freshly wading into these waters. Progress in midface surgery has been retarded by past paradigms of lower eyelid surgery. Specifically, addressing many of the deficiencies of the midface requires that the surgeon necessarily correct midface bone changes as well as involutional midface soft tissue changes. Until recently, the adult projection of the maxilla was considered static, except in cases of trauma. An individual either had good projection of the cheek bones or an anatomic variant with hypoplastic projection (1). Recent studies have demonstrated that over time the adult maxillary face and orbital rim retrudes and inferiorly rotates (2, 3, 4, 5 and 6). It is not clear if these changes are simply the result of long-term bone remodeling or if osteoporosis also contributes to bone loss at the orbital rim. What is clear in our patients is that, after the mid-20 years, maxillary hypoplasia becomes an increasingly prevalent feature of the aging face. As an individual enters his/her 40s, midface soft tissue ptosis often is manifested by a pronounced nasojugal groove defined inferiorly by the leading edge of the ptotic malar fat pad and typically superiorly by lower eyelid fullness from pseudoherniated orbital fat (Fig. 4.5.1).
Lower eyelid surgery has primarily addressed soft tissue with lateral canthal, skin, and fat procedures including transcutaneous and transconjunctival lower blepharoplasty. Even the elaborate “Madame Butterfly” procedure developed by Shorr only horizontally and vertically lengthens the surgically compromised eyelid but ultimately does not restore volume to the midface-lower eyelid complex (7). Dissatisfaction with the results of these techniques has spurred surgeons to explore new methods to address the scope of lower eyelid and midface abnormalities. Midface ptosis is not simply an aesthetic deficit. It also profoundly affects almost all
aspects of lower eyelid reconstruction, which is enormously more difficult in the setting of a prominent globe (3,6,8). Because soft tissue is only part of the picture, failure to understand the important role of facial skeletal remodeling at the orbital rim has severely limited the surgeon’s ability to repair midface ptosis by soft tissue technique alone (Fig. 4.5.2) (9).
aspects of lower eyelid reconstruction, which is enormously more difficult in the setting of a prominent globe (3,6,8). Because soft tissue is only part of the picture, failure to understand the important role of facial skeletal remodeling at the orbital rim has severely limited the surgeon’s ability to repair midface ptosis by soft tissue technique alone (Fig. 4.5.2) (9).
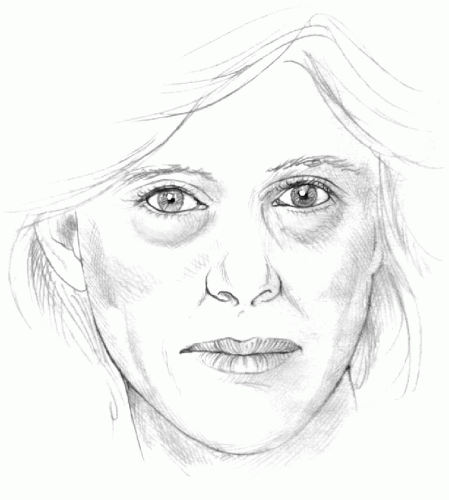 Figure 4.5.1. Midface ptosis often is manifested by a pronounced nasojugal groove defined inferiorly by the leading edge of the ptotic malar fat pad and superiorly by lower eyelid fullness from pseudoherniated orbital fat. |
Early midface work by Hamra, Owsley, and others relied on elevating the malar fat pad laterally or superolaterally through a face lift approach with the aim of reducing the nasolabial fold and secondarily the nasojugal groove (10, 11, 12 and 13). Other authors described the elevation of midface tissues in a superotemporal approach via a coronal or a more limited temple incision (14, 15 and 16). With the adoption of the
endoscopic forehead lift, techniques for superotemporal midface lifting via an endoscopic approach were described and popularized, including the so-called coronocanthoplasty (17, 18 and 19). Alternative methods to accomplish a similar midface lift through an extended infracilary incision also have been described (20, 21 and 22). These techniques have the virtue of offering the surgeon sites for substantial and reliable fixation of the lifted malar soft tissue to either the temporalis fascia superotemporally or the preparotid fascia laterally. More recently, minimally invasive cabling techniques have been introduced (23,24). However, midface lifts that pull the malar soft tissue laterally or superolaterally result in a subtly unnatural vector of lift. The reason for this is simple: the midface soft tissue falls in more of a vertical vector and less so in an inferior medial direction.
endoscopic forehead lift, techniques for superotemporal midface lifting via an endoscopic approach were described and popularized, including the so-called coronocanthoplasty (17, 18 and 19). Alternative methods to accomplish a similar midface lift through an extended infracilary incision also have been described (20, 21 and 22). These techniques have the virtue of offering the surgeon sites for substantial and reliable fixation of the lifted malar soft tissue to either the temporalis fascia superotemporally or the preparotid fascia laterally. More recently, minimally invasive cabling techniques have been introduced (23,24). However, midface lifts that pull the malar soft tissue laterally or superolaterally result in a subtly unnatural vector of lift. The reason for this is simple: the midface soft tissue falls in more of a vertical vector and less so in an inferior medial direction.
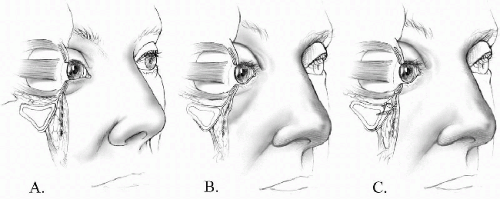 Figure 4.5.2. Three-quarter cutaway profiles of the midface. A:Youthful profile. Notice the projection of the orbital rim and the presence of subcutaneous fat anterior to the orbicularis oculi muscle at the orbital rim. B: Mature profile. Notice the loss of orbital rim projection and retrusion of the malar face. There is descent of the malar fat pad including the subcutaneous fat. C: Surgically corrected profile. The e-PTFE implant is held in place by microscrews correcting the loss of projection at the orbital rim. The superior edge of the implant provides a strong site for suture fixation of the advanced cheek soft tissues. (From Steinsapir KD. Aesthetic and restorative midface lifting with hand-carved, expanded polytetrafluoroethylene orbital rim implants. Plast Reconstr Surg 2003; 111:1727-1737, with permission.) |
Shorr and co-workers advocate the vertical elevation of the midface soft tissues to their site of origin with the goal of reestablishing a more youthful midface contour (25,26). Laxity of the osteocutaneous ligaments that support the midface soft tissues, including the orbitomalar, zygomatic, and masseteric cutaneous ligaments, appear to be important factors in the descent of the subcutaneous tissues of the midface (27). The vertical midface lift essentially reestablishes the relationship of the malar fat to the orbital rim before the attenuation of these ligaments. Vertical elevation of the midface soft tissues to the orbital rim requires fixating mobilized suborbicularis oculi fat and midface soft tissues to the diaphanous inferior orbital arcus marginalis and orbital rim periosteal tissues. Unfortunately, the arcus marginalis is flimsy and insubstantial, and it lacks the strength to reliably hold the sutures needed to support the midface soft tissues while a permanent scar forms. The vertical soft tissue midface lift also does not address the involutional loss of bone projection at the orbital rim and malar face (9).
Other methods have been described to address midface deficits. Cheek implants represent a classic approach to midface deficiencies. However, cheek augmentation often only exaggerates the nasojugal groove (28). Flowers (1) described the placement of a comma-shaped silicone implant extending from the orbital rim down over the malar face. The implant is notched to accommodate the inferior orbital neurovascular bundle. More recently, a porous polyethylene implant has been used to accomplish the same augmentation (29). Loeb (30,31) originally described the arcus marginalis release with placement of the inferior orbital fat onto the orbital rim as a vascular pedicle graft to help fill in the nasojugal groove. This surgery was popularized by Hamra (32) and subsequently by Goldberg (33,34). However, this technique provided only a modest improvement in the nasojugal groove, but importantly it removes volume from the lower eyelid.
To address the limitations of prior techniques, since 1998 I have used hand-carved reinforced sheets of expanded polytetrafluoroethylene (e-PTFE; W.L. Gore & Associates, Flagstaff, AZ) to compensate for the loss of bone projection at the orbital rim and maxillary face (9). This material is readily available in suitable sizes and thickness, and it can be carved to size and shape to compensate for deficiencies in projection of the orbital rim and malar face. The material is physically strong yet pliable, so it can be inserted with limited exposure. With the implant firmly anchored to the bone using titanium microscrews, the advanced midface soft tissues can be securely sutured to the e-PTFE implant at the orbital rim for lasting fixation (Figs. 4.5.1 and 4.5.3). This innovation has solved two important challenges to successful vertical midface lifting: restoration of underlying orbital rim projection, and reliable support and fixation of the vertically lifted midface soft tissues.
With this foundation, several controversies in midface surgery can be addressed. Early descriptions of the midface lift emphasized the lifting of the suborbicularis oculi fat pad (SOOF). Some authors on the subject were ambiguous regarding the relationship among the malar fat pad, the SOOF, and the superficial musculoaponeurotic system (SMAS). Anatomic studies have demonstrated that the SMAS is discontinuous in the midface (27). Consequently, there is no anatomic separation between the SOOF and the malar fat pad. The SOOF is simply the
deeper continuation of the malar fat pad, which invests the lip elevators as they insert on the malar face below the orbital rim. The SOOF component is closely adherent to the periosteum and does not play a significant role in midface ptosis. The balance of the malar fat pad in youth is firmly held to the orbital rim by the orbitomalar ligament. With age, there is attenuation of the orbitomalar and zygomatic ligaments, which causes the bulk of the malar fat pad to become ptotic. As already discussed, this is superimposed on involutional changes in the projection of the orbital rim and malar face.
deeper continuation of the malar fat pad, which invests the lip elevators as they insert on the malar face below the orbital rim. The SOOF component is closely adherent to the periosteum and does not play a significant role in midface ptosis. The balance of the malar fat pad in youth is firmly held to the orbital rim by the orbitomalar ligament. With age, there is attenuation of the orbitomalar and zygomatic ligaments, which causes the bulk of the malar fat pad to become ptotic. As already discussed, this is superimposed on involutional changes in the projection of the orbital rim and malar face.
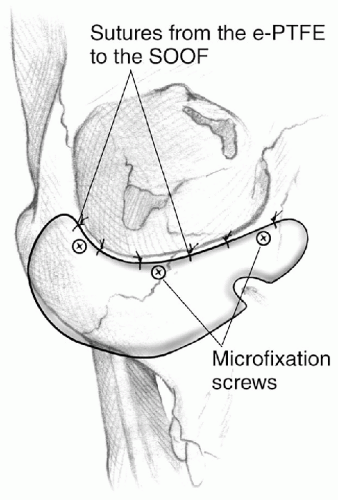 Figure 4.5.3. Sketch indicating how the carved e-PTFE implant is fixated to the orbital rim. (From Steinsapir KD. Aesthetic and restorative midface lifting with hand-carved, expanded polytetrafluoroethylene orbital rim implants. Plast Reconstr Surg 2003;111:1727-1737, with permission.) |
If one were to rely on early descriptions of the SOOF, one might wrongly excise this fat or attempt to lift this structure without adequate mobilization (26,35). It must be appreciated that the so-called preperiosteal SOOF lift is a misnomer. It actually represents a retro-orbicularis oculi dissection into the bulk of the malar fat overlying the lip elevators. Care must be taken in dissecting under the orbicularis oculi muscle to avoid denervation (36). This generally means limited gentle vertical spreading sufficient to accomplish the desired tissue advancement. Only modest tissue advancement can be accomplished in this plane. However, this approach is more than adequate for the recruitment of skin and dynamic orbicularis oculi muscle necessary for neoclassic post-Mohs cancer surgery reconstruction. This technique has a role in the armamentarium of the oculoplastic surgeon.
The subperiosteal midface lift with a wide release of the periosteum with or without periosteotomy is needed when a more powerful midface lift is required (9). This approach can be used as an alternative to an atonic Mustarde flap for reconstruction of a large lower eyelid defect by mobilizing the cheek medially with a subperiosteal dissection over the zygomatic arch and on to the masseter fascia. Only a limited rejuvenation of the midface is possible when the midface soft tissue is resuspended to the orbital rim without augmenting the orbital rim. However, when full-thickness midface advancement is performed in conjunction with e-PFTE orbital rim implant, truly impressive midface rejuvenation is possible (Fig. 4.5.4).
This technique can be combined with a hard palate or acellular dermal spacer graft to the lower eyelid when necessary. Routinely, cosmetic midface lift over a hand-carved e-PFTE orbital rim implant is performed bilaterally and in conjunction with upper blepharoplasty, endoscopic forehead lifting, and facial rhytidectomy (Fig. 4.5.5).
This technique can be combined with a hard palate or acellular dermal spacer graft to the lower eyelid when necessary. Routinely, cosmetic midface lift over a hand-carved e-PFTE orbital rim implant is performed bilaterally and in conjunction with upper blepharoplasty, endoscopic forehead lifting, and facial rhytidectomy (Fig. 4.5.5).
 Figure 4.5.4. A: A 51-year-old man with midface ptosis, pseudoherniated orbital fat, and lower eyelid rhytides. B: Six months after surgery, the patient had a bilateral midface lift over hand-carved e-PTFE orbital rim implants. A lower eyelid chemical peel also was performed. Note that no lower eyelid fat was removed. |
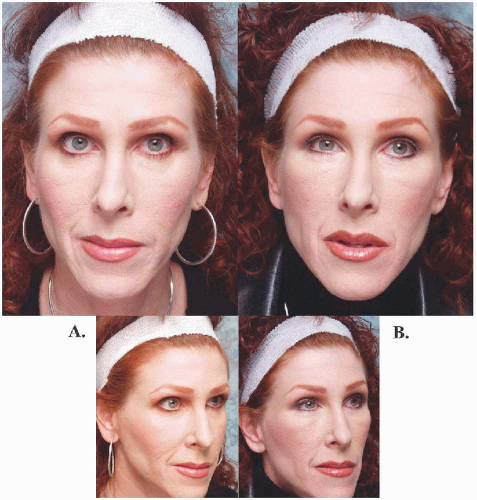 Figure 4.5.5. A: A 43-year-old woman with midface and brow ptosis. B: Eight months after simultaneous bilateral midface lift over hand-carved e-PTFE orbital rim implants and endoscopic forehead lift. |
It is not routinely necessary to patch the eye following midface surgery. In cases where it is necessary to use a hard palate graft, surgery is performed one eye at a time with the eye closed for a week with Frost sutures. However, in cases where only a small degree of lower eyelid elevation is needed, an acellular dermal graft can be used as a temporary spacer graft without the need to close the lid with Frost sutures for traction.
In summary, midface surgery is now an essential part of oculoplastic surgery. The midface can be widely accessed through a very limited skin incision using a swinging eyelid approach. To use this approach, the surgeon must be comfortable with the lateral canthoplasty. These soft tissue techniques provide the access needed to safely and predictably augment the orbital rim with one of a number of implant materials, including hand-carved reinforced sheets of e-PFTE. This latter material can be fixated to the orbital rim with microscrews to create a substantial and permanent anchor for vertically lift midface soft tissues. This procedure creates for the first time a means to comprehensively rejuvenate and reconstruct the midface region.
References
1. Flowers RS. Tear trough implants for correction of tear trough deformity. Clin Plast Surg 1993; 20:403-415.
2. Pessa JE, Zadoo VP, Mutimer KL, et al. Relative maxillary retrusion as a natural consequence of aging: combining skeletal and soft-tissue changes into an integrated model of midfacial aging. Plast Reconstr Surg 1998;102:205-212.
3. Pessa JE. An algorithm of facial aging: verification of Lambros’s theory by three-dimensional stereolithography, with reference to the pathogenesis of midfacial aging, scleral show, and the lateral suborbital trough deformity. Plast Reconstr Surg 2000;106:479-488.
4. Zadoo VP, Pessa JE. Biological arches and changes to the curvilinear form of the aging maxilla. Plast Reconstr Surg 2000;106:460-468.
5. Bartlett SP, Grossman R, Whitaker LA. Age-related changes of the craniofacial skeleton: an anthropometric and histologic analysis. Plast Reconstr Surg 1992;90:592-600.
6. Goldberg R, Relan A, Hoenig J. Relationship of the eye to the bony orbit, with clinical correlations. Aust N Z J Ophthalmol 1999;27:398-403.
7. Shorr N. Madame butterfly procedure with hard palate graft: management of postblepharoplasty round eye and scleral show. Facial Plast Surg 1994;10:90-118.
8. Steinsapir KD, Shorr N. Suborbital augmentation. In: Bosniak S, ed.Principles and practice of ophthalmic plastic and reconstructive surgery, vol. 1. Philadelphia: WB Saunders, 1996.
9. Steinsapir KD. Aesthetic and restorative midface lifting with hand-carved, expanded polytetrafluoroethylene orbital rim implants. Plast Reconstr Surg 2003;111:1727-1737.
10. Owsley JQ. Elevation of the malar fat pad superficial to the orbicularis oculi muscle for correction of prominent nasolabial folds. Clin Plast Surg 1995;22:279-293.
11. Owsley JQ. Lifting the malar fat pad for correction of prominent nasolabial folds. Plast Reconstr Surg 1993;91:463-474.
12. Hamra ST. Composite rhytidectomy. Plast Reconstr Surg 1992;90:1-13.
13. Keller GS, Cray J. Suprafibromuscular facelifting with periosteal suspension of the superficial musculoaponeurotic system and fat pad of Bichat rotation. Arch Otolaryngol Head Neck Surg 1996;122:377-384.
14. Dempsey PD, Oneal RM, Izenberg PH. Subperiosteal brow and midface lifts. Aesthetic Plast Surg 1995;19:59-68.
15. Collawan SS, Vasconez LO, Gamboa M, et al. Subcutaneous approach for elevation of the malar fat pad throughout a prehairline incision. Plast Reconstr Surg 1996;97:836-841.
16. Hagerty RC. Central suspension technique of the midface. Plast Reconstr Surg 1995;96: 728-730.
17. Turk J, Goldman A. SOOF lift and lateral retinacular canthoplasty. Facial Plast Surg 2001;17: 37-48.
18. Sullivan SA, Dailey RA. Endoscopic subperiosteal midface lift: surgical technique with indications and outcomes. Ophthal Plast Reconstr Surg 2002;18:319-330.
19. Freeman MS. Endoscopic techniques for rejuvenation of the midface. Facial Plast Surg Clin North Am 2001;9:453-468.
20. McCord CD, Codner MA, Hester TR. Redraping the inferior orbicularis arc. Plast Reconstr Surg 1998;102:247-249.
21. Hester TR, Codner MA, McCord CD, et al. Evolution of technique of the direct transblepharoplasty approach for the correction of lower lid and midface aging: maximizing results and minimizing complications in a 5-year experience. Plast Reconstr Surg 2000;105:393-406.
22. Moellenken B. The superficial subciliary cheek lift, a technique for rejuvenating the infraorbital region and nasojugal groove: a clinical series of 71 patients. Plast Reconstr Surg 1999; 104:1863-1874.
23. Sasaki GH, Cohen AT. Meloplication of the malar fat pads by percutaneous cable-suture technique for midface rejuvenation: outcome study (392 cases, 6 years’ experience). Plast Reconstr Surg 2002;110:635-654.
24. Yousif NJ, Matloub MD, Summers AN. The midface sling: a new technique to rejuvenate the midface. Plast Reconstr Surg 2002;110:1541-1543.
25. Hoenig JA, Shorr N, Shorr J. The suborbicularis oculi fat in aesthetic and reconstructive surgery. Int Ophthalmol Clin 1997;37:179-191.
26. Edlestein C, Balch K, Shorr N, et al. The transeyelid subperiosteal midface-lift in the unhappy postblepharoplasty patient. Semin Ophthalmol 1998;13:103-106.
27. Lucarelli MJ, Khwarg SI, Lemke BN, et al. The anatomy of midfacial ptosis. Ophthal Plast Reconstr Surg 2000;16:7-22.
28. Hamra ST. Arcus marginalis release and orbital fact preservation in midface rejuvenation. Plast Reconstr Surg 1995;96:354-362.
29. Yaremchuk MJ. Infraorbital rim augmentation. Plast Reconstr Surg 2001;107:1585-1592.
30. Loeb R. Fat pad sliding and fat grafting for leveling lid depressions. Clin Plast Surg 1981;8: 757-776.
31. Loeb R. Naso-jugal groove leveling with fat tissue. Clin Plast Surg 1993;20:393-400.
32. Hamra ST. The role of orbital fat preservation in facial aesthetic surgery: a new concept. Clin Plast Surg 1996;23:17-28.
33. Goldberg R. Transconjunctival orbital fat repositioning: transposition of orbital fat pedicles into a subperiosteal pocket. Plast Reconstr Surg 2000;105:743-748.
34. Goldberg R, Edelstein C, Shorr N. Fat repositioning in lower blepharoplasty to maintain infraorbital rim contour. Facial Plast Surg 1999;15:225-229.
35. Aiache AE, Ramirez OH. The suborbicularis oculi fat pads: an anatomic and clinical study. Plast Reconstr Surg 1995;95:37-42.
36. Hwang K, Lee DK, Lee EJ, et al. Innervation of the lower eyelid in relation to blepharoplasty and midface lift: clinical observation and cadaveric study. Ann Plast Surg 2001;47:1-7.
EXPERT COMMENTARY
Robert Glasgold
Mark Glasgold
The midface, which consists of the lower eye and cheek, is the first facial area to show aging changes in the majority of our patients. Patients often begin detecting these changes in their mid-30s and usually come in complaining of bags under the eyes or a deepening nasolabial fold. Although it is important to address these specific concerns, we also must be aware of the larger issue of midfacial aging: the loss of the youthful continuous convexity of the cheek-lower eyelid complex (Fig. 4.5.6).
Upon examination of these patients, we see in the periorbital region there is hollowing over the orbital rim and pseudoherniation of orbital fat, a deepened nasojugal groove, and a break of the cheek-lower eyelid convexity. In the midcheek, a malar depression (Fig. 4.5.6) develops, running parallel to the nasolabial fold, and there is a deepening of the nasolabial fold. These changes result in a double-peak contour to the cheek, which is the hallmark of midfacial aging.
The manifestations of aging in the midface are the result of two processes. First and most important is loss of midface volume due to involution of the skeletal and soft tissue framework. Second is gravitational ptosis.
Rejuvenation of the midface requires correction of these two processes. Lifting procedures have received the most attention in the literature, but we agree with Steinsapir that without volume replacement, lifting alone is of limited value in most patients.
Rejuvenation of the midface requires correction of these two processes. Lifting procedures have received the most attention in the literature, but we agree with Steinsapir that without volume replacement, lifting alone is of limited value in most patients.
 Figure 4.5.6. Left: Young patient demonstrates youthful continuous contour of the lower eye cheek. Right: Aging patient demonstrates orbital hollowing, midface depression, and double-peak contour of the midface. |
Our early experience with midfacial rejuvenation focused primarily on lifting procedures in an attempt to elevate ptotic malar fat pads and SOOF. We have used endoscopic subperiosteal midface lifts, subciliary extended blepharoplasty, deep plane face lifting with suspension sutures, and percutaneous suspension sutures. Endoscopic subperiosteal lifting elevates the entire cheek mass and can have a nice effect on hollowing of the orbital rim. This procedure does not address ptosis of the subcutaneous malar fat pad in relation to the underlying facial musculature and has no effect on the malar depression, the trough that extends from the nasojugal groove through the cheek between the malar fat pad and the zygomatic arch. It also produces significant postoperative swelling for the limited amount of correction it achieves.
Deep plane face lifting as described by Hamra (1) directly lifts the malar fat pad in a superior lateral direction. Our experience, which reflects that of Hamra, is that there is little real effect of malar fat positioning on the nasolabial fold. Our experience with suture suspension as described by Owsley was unsatisfactory due to the difficulty in avoiding dimpling with suture placement. Subciliary lifting procedures have a significant incidence of lower lid malposition, pose the problem of redraping a large amount of skin through the extended incision, and have a prolonged recovery period (2). Finally, we have not been impressed with our long-term results (greater than 2 years) in correcting orbital hollowing by mobilization and transfer of orbital fat. In general, the filling that can be achieved with this mobilization is inadequate to correct the amount of volume depletion in this area.
The procedure described by Steinsapir correctly focuses on what we believe are the two key components of midfacial rejuvenation. He addresses
the hollowing of both the midface and orbital rim with e-PTFE implants and uses a subperiosteal subciliary midface lift to correct gravitational changes. Our primary concerns with this procedure are the learning curve for carving the implants and the potential for lower lid malposition due to scarring of the middle lamella with the subciliary lift.
the hollowing of both the midface and orbital rim with e-PTFE implants and uses a subperiosteal subciliary midface lift to correct gravitational changes. Our primary concerns with this procedure are the learning curve for carving the implants and the potential for lower lid malposition due to scarring of the middle lamella with the subciliary lift.
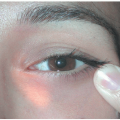
Our current approach to midface rejuvenation combines the use of a percutaneous suture suspension technique and fat autografting (3,4). The percutaneous suture suspension is a simple procedure that directly lifts the cheek fat pad, with minimal morbidity or potential complications. The procedure involves a small temporal incision with elevation in an anterior and inferior direction along the deep temporal fascia. Dissection is carried out to approximately the lateral canthus and the sentinel vein, which, if visualized, is cauterized with a bipolar cautery. Using a straight needle, a guiding 3.0 vicryl suture (polyglactin, Ethicon, Somerset, NJ) along with a 4.0 prolene suture (Ethicon) threaded through a 2mm piece of Gore-Tex, are passed from the puncture hole in the cheek to the previously dissected temporal pocket (Fig. 4.5.7). The Vicryl suture is pulled in a sawing motion to release puckering of the overlying skin. The Vicryl suture is removed, and the Prolene suture is pulled with the Gore-Tex anchor to elevate the malar fat pad. The two ends of the Prolene are then sutured to the deep temporal fascia (Fig. 4.5.8). This is repeated through a second puncture site on the same side. We use this technique to address ptosis of the malar fat pads and have found it to be effective in patients with good midface volume or heavy nasolabial
folds. This procedure, similar to most lifting techniques, is unable to correct the midface depression or orbital hollowing in patients who need volume. We use fat autografting for volume replacement in the aging face because it allows the periorbital and cheek region to be treated as a single continuous unit.
folds. This procedure, similar to most lifting techniques, is unable to correct the midface depression or orbital hollowing in patients who need volume. We use fat autografting for volume replacement in the aging face because it allows the periorbital and cheek region to be treated as a single continuous unit.
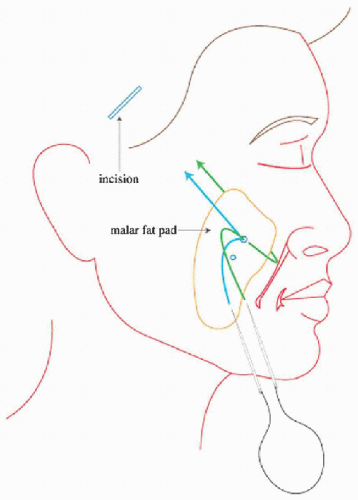 Figure 4.5.7. Keith needles threaded with Vicryl and Prolene sutures are passed around the malar fat pad and up through the temple incision. |
 Figure 4.5.8. Malar fat pad is suspended by Prolene suture to deep temporal fascia. |
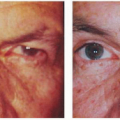
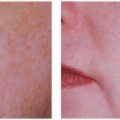
 Figure 4.5.9. Patient before and 3 weeks after percutaneous cheek lift and autologous fat transfer. |
Our technique of fat transfer to the midface incorporates two popular approaches: lipostructure as taught by Dr. Sidney Coleman (5) and fat autograft muscle injection (FAMI) as taught by Dr. Roger Amar (personal communication, 2002). Lipostructure is excellent for filling in areas such as the nasojugal groove and midface depression; however, it often results in significant bruising and swelling. The FAMI technique produces less bruising and
is very effective in the orbital rim, cheek, and buccal regions. By using a combination of techniques, we get a more complete filling while minimizing morbidity. The technical aspects of fat autografting are critical to its success, and invariably its critics use incorrect methods. The technique is readily learnable, and we highly recommend taking one of the extensive courses offered by Coleman or Amar or studying with a physician who has significant experience. Without proper training, physician satisfaction with the procedure is poor.
is very effective in the orbital rim, cheek, and buccal regions. By using a combination of techniques, we get a more complete filling while minimizing morbidity. The technical aspects of fat autografting are critical to its success, and invariably its critics use incorrect methods. The technique is readily learnable, and we highly recommend taking one of the extensive courses offered by Coleman or Amar or studying with a physician who has significant experience. Without proper training, physician satisfaction with the procedure is poor.
 Figure 4.5.10. Patient before and 1 year after percutaneous cheek lift and autologous fat transfer. |
The majority of our patients seeking midfacial rejuvenation will undergo the combination of fat autografting to the cheek and orbital rim combined with percutaneous cheek lift (Figs. 4.5.9 and 4.5.10). The fat autograft is done first, followed by the cheek lift. At the end of the procedure we usually place a bit of fat over the suture insertion sites to prevent dimpling. The procedure is done with conscious sedation on an outpatient basis. We have observed one hematoma and no nerve complications in our experience with this procedure over the past 2 years.
References
1. Hamra ST. A study of the long-term effect of malar fat repositioning in face lift surgery: short-term success but long-term failure. Plast Reconstr Surg 2002;110:940-951.
2. Hester TR, Codner MA, McCord CD, et al. Evolution of technique of the direct transblepharoplasty approach for the correction of lower lid and midfacial aging: maximizing results and minimizing complications in a 5-year experience. Plast Reconstr Surg 2000;105:393-406.
3. Kelller GS, Namazie A, Blackwell K, et al. Elevation of the malar fat pad with a percutaneous technique. Arch Facial Plastic Surg 2002;4:20-25.
4. Sasaki GH, Cohen AT. Meloplication of the malar fat pad by percutaneous cable-suture technique for midface rejuvenation: outcome study (392 cases, 6 years’ experience). Plast Reconstr Surg 2002;110:635-654.
5. Coleman SR. Facial recontouring with liposculpture. Clin Plast Surg 1997;24:347-367.
EDITORIAL COMMENTARY
The issue of lid malpositions after subciliary lifting procedures is raised by Drs. Glasgold and Glasgold. Of critical value is stabilization of the lateral canthal tissues and lower eyelid and proper suspension of the eyelid tissues.This subject was discussed in a personal communication by Drs. McCord and Hester. They requested that the following statement be published.
EXPERT COMMENTARY
Clinton D. McCord
T. Roderick Hester Jr.
A few years ago we reviewed our previous 5-year experience with cheek lift procedures and reported an overall revision rate (any kind of revision, including skin fold trim, cyst removal) of 18% (1). Revision for lower lid malposition was only less than 4%. Because of misquotations and the flak that it created and to set the record straight, in 1999 to 2001 we each reviewed a 1.5-year series of our more recent cases and included as revisions only those with lower lid malposition, for a revision rate of less than 2% (for lower lid
malposition). This magnitude of revision rate is well within the acceptable range for any cosmetic procedure.
malposition). This magnitude of revision rate is well within the acceptable range for any cosmetic procedure.
The initial problems that individuals outside our practice were having with lower lid malposition following a cheek lift had nothing to do with the subciliary incision, the subperiosteal dissection, or the redraping of the eyelid-cheek skin. The problems that occurred were the result of failure to properly anchor the lateral canthus or the inferior arc of orbicularis. It has been our experience that canthal anchoring is necessary to maintain eye fissure shape and prevent lower lid malposition. Very secure anchoring of the inferior arc of the orbicularis (which is the “handle” of the cheek lift) is needed to support the cheek and helps to maintain lower lid position. We refer the readers to our publications (2,3).
References
1. Hester TR, Codner MA, McCord CD, et al. Evolution of technique of the direct transblepharoplasty approach for the correction of lower lid and midfacial aging: maximizing results and minimizing complications in a 5-year experience. Plast Reconstr Surg 2000;105:393-406.
2. McCord CD, Codner MA, Hester TR. Redraping the inferior orbicularis arc. Plast Reconstr Surg 1998;102:2471-2479.
3. McCord CD, Boswell CB, Hester TR. Lateral canthal anchoring. Plast Reconstr Surg 2003; 112:222-237.
EDITORIAL COMMENTARY
McCord et al. (1) determined that the so-called inner canthal orbicularis deep heads are responsible for maintenance of proper eyelid position and normal tone and blinking. In contrast, the so-called extracanthal orbicularis muscles play a small role in casual blinking, lower lid position, and the lacrimal pump mechanism. Lateral canthal stability assures that blinking results in a vertical direction of contracture that closes the eyelids. Poor stabilization of the lateral canthal creates a nasal vector upon orbicularis muscle contraction.
Surgical placement of the lateral canthus can be guided by the shape of the palpebral fissure and by the relationship of the lateral canthus to the pupil. The lateral scleral triangle normally is larger and wider than the nasal scleral triangle.The lateral canthus should be positioned at the level of the inferior edge of the pupil and inside the lateral orbital rim in patients with Hertel exophthalmometry readings of 15 to 17 mm. In patients with deep-set eyes (Hertel measurements less than 15 mm), fixation should be more internal and less superior to avoid “upward clotheslining” of the lower lid and consequent reduction of the size of the lateral scleral triangle. In patients with prominent eyes with Hertel measurements of 18 mm or greater, the fixation is shifted upward to proven the downward clotheslining effect.
Reference
1. McCord CD, Boswell CB, Hester TR. Lateral canthal anchoring. Plast Reconstr Surg 2003;112: 222-237.
EXPERT COMMENTARY
Chee-Chew Yip
John D. McCann
The midface is an important anatomic region of the face, and aging changes pose functional and aesthetic concerns to the patient. The aging midface is characterized by cheek descent, prominent nasolabial fold, exaggerated nasojugal fold, and flattening of the infraorbital region (1). The anatomic changes in midface ptosis are related to attenuation of the orbitofacial retaining ligaments (such as the orbitomalar and zygomatic ligaments) causing a loss of structural support for the facial skin and subcutaneous tissue (2,3). In addition, loss of skin elasticity, subcutaneous fat deflation, and diminution of bony projection of the inferior orbital rim and maxilla (4, 5 and 6
 Preoperative Evaluation of Patients Undergoing Cosmetic Blepharoplasty
Preoperative Evaluation of Patients Undergoing Cosmetic Blepharoplasty
 Role of Chemical Peels and Other Superficial Resurfacing Procedures
Role of Chemical Peels and Other Superficial Resurfacing Procedures
 Fat Repositioning in Transconjunctival Lower Eyelid Blepharoplasty
Fat Repositioning in Transconjunctival Lower Eyelid Blepharoplasty
 Endoscopic Brow Lift
Endoscopic Brow Lift
 Hyaluronic Acid and Other Soft Tissue Fillers for Facial Rejuvenation
Hyaluronic Acid and Other Soft Tissue Fillers for Facial Rejuvenation
 Infraorbital Discoloration: Dark Circles—An Anatomic Analysis and Treatment
Infraorbital Discoloration: Dark Circles—An Anatomic Analysis and Treatment




Related posts:
Preoperative Evaluation of Patients Undergoing Cosmetic Blepharoplasty
Role of Chemical Peels and Other Superficial Resurfacing Procedures
Fat Repositioning in Transconjunctival Lower Eyelid Blepharoplasty
Endoscopic Brow Lift
Hyaluronic Acid and Other Soft Tissue Fillers for Facial Rejuvenation
Infraorbital Discoloration: Dark Circles—An Anatomic Analysis and Treatment
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
