The explosion of interest in chemical peeling and laser resurfacing on the part of dermatologists and cosmetic surgeons has paralleled the general public’s interest in acquiring a youthful appearance by rehabilitating photoaged skin. The public’s interest has been heightened further by advertising for cosmetic agents, over-the-counter chemicals, and treatment programs that have entered the general market of products meant to rejuvenate skin and erase the marks of sun damage and age. Most of these over-the-counter home do-it-yourself programs have been tried by patients, and by the time they consult their plastic surgeon, cosmetic surgeon, or dermatologist, they are ready for a more definitive procedure performed with either chemical peeling or laser resurfacing. It is the obligation of the physician to analyze the patient’s skin type and degree of photoaging skin, and thus prescribe the correct facial rejuvenation procedure that will provide the greatest benefit for the least risk factors and morbidity. The cosmetic surgeon should have available for his/her consumer the options of medical or cosmeceutical topical therapy, dermabrasion, chemical peeling, and lasers available for selective skin destruction and resurfacing. Each of these techniques maintains a place in the armamentarium of the cosmetic surgeon to provide the appropriate treatment for each individual patient and his/her specific problem.
The approach to photoaging skin has expanded beyond a one-stage procedure to now include preparatory medical therapy and posttreatment cosmeceutical topical therapy to maintain results and prevent further photodamage. Thus, the dermatologist’s and cosmetic surgeon’s office has become not only a surgical treatment session but also an educational setting for skin protection and care and a marketplace for the patient to obtain the necessary topicals for skin protection. It is up to the dermatologist, cosmetic surgeon, and plastic surgeon to fully understand the nature of skin and sun damage, the protective techniques available, and the active agents that work as cosmeceutical preparations. Having available multiple procedures to solve these problems will make his/her patients better candidates for the right procedure to restore and rehabilitate their skin.
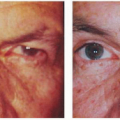
Chemical peeling involves the application of a chemical exfoliant to wound the epidermis and dermis for the removal of superficial lesions and improvement of skin texture. Various acidic and basic chemical agents are used to produce the varying effects of light to medium to deep chemical peels through differences in their ability to destroy skin. The levels of penetration, destruction, and inflammation determine the level of peeling. Light superficial peel consists of stimulation of epidermal growth through removal of the stratum corneum without necrosis. Through exfoliation, it thickens the epidermis with qualitative regenerative changes. A full superficial chemical peel consists of destruction of the epidermis inducing the regeneration of the epidermis. Further destruction of the epidermis and induction of inflammation within the papillary dermis constitute a medium depth peel (
1). Further inflammatory response in the deep reticular dermis induces new collagen production and ground substances, which constitutes a deep chemical peel. These now have been well classified, and usage has been categorized for various degenerative conditions associated with photoaging skin based on levels of penetration. Thus, the physician has tools capable of solving problems that may be mild, moderate, or severe with agents that are very superficial, superficial, medium depth, and deep peeling chemicals. The physician must choose the right agent for each patient and condition.
Indications and Patient Selection
Analyzing the patient with photoaging skin must take into account skin color and type, and the degree of photoaging. Various classification systems are available, and I would like to present a combination of three systems that would simplify and help the physician define the right program or therapeutic procedure for his/her patient. The Fitzpatrick skin type system classifies degrees of pigmentation and ability to tan using grades I to VI. It prognosticates sun sensitivity, susceptibility to photodamage, and ability for facultative melanogenesis (one’s intrinsic ability to tan) (
2). In addition, this system classifies skin with regard to its risk factors for complications during chemical peeling. Fitzpatrick divides skin types into grades I through VI, taking into account both color and reaction to the sun. Skin types I and II are pale white and freckled, with a high degree of potential to burn with sun exposure. Types III and IV can burn but usually are an olive to brown coloration. Types V and VI are dark brown to black skin that rarely ever burns and usually does not require sunscreen protection (
Table 4.3.1). The patient with type I or II skin with significant photodamage needs regular sunscreen protection prior to and after the procedure. Such a patient, however, has little risk for hypopigmentation or reactive hyperpigmentation after a chemical peeling procedure. The patient with type III through VI skin has a greater risk for pigmentary dyschromia—hyperpigmentation or hypopigmentation—after a chemical peel and may need pretreatment
and posttreatment with both sunscreen and bleaching to prevent these complications (
3). Pigmentary risks are generally not a great problem with very superficial and superficial chemical peeling, but they may become a significant problem with medium and deep chemical peeling.
The Glogau system classifies severity of photodamage, taking into account the degree of epidermal and dermal degenerative effects (
4). Categorization is graded I to IV, ranging from mild, moderate, advanced, to severe photodamaged skin. These categories are devised for therapeutic intervention. Category I in young individuals or minimal degree photodamage should be treated with light chemical peeling and medial treatment. Categories II and III would entail medium depth chemical peeling. Category IV would need the modalities listed plus cosmetic surgical intervention for gravitational changes (
Table 4.3.2).
Monheit and Fulton have devised a system for quantitating photodamage and have developed numerical scores that would fit into corresponding rejuvenation programs (
5). In analyzing photodamage, the major categories include epidermal color with skin lesions and dermal with textural changes. Dermal changes include wrinkles, cross-hatched lines, sallow color, leathery appearance, crinkly thin parchment skin, and the pebblish white nodules of milia. Each of these is classified, giving the patient a point score from 1 to 4. In addition, the number and extent of lesions are categorized from freckles, lentigines, telangiectasias, actinic and seborrheic keratoses, skin cancers, and senile comedones. These also are added in a classification system scored 1 to 4, and the final score results are tabulated. A total score of 1 to 4 indicates very mild damage, and the patient would adequately respond to a five-step skin care program including sunscreen protection, retinoic acid, glycolic acid peels, and selective lesional removal. A score of 5 to 9 includes all of the program for a total score of 1 to 4 plus repetitive superficial peeling agent programs such as glycolic acid, Jessner solution, or lactic acid peels. A score of 10 to 14 includes medium depth chemical peeling, and a score of 15 or above includes deep chemical peeling or laser resurfacing. Thus, during the consultation the patient can understand his/her degree of photodamage and the necessity for an individual peeling program (
Table 4.3.3) (
6,
7).
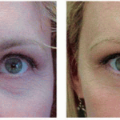
The chief indications for chemical peeling are associated with reversal of actinic changes, such as photodamage, rhytides, actinic growths, pigmentary dyschromias, and acne scars (
4). The physician thus can use his/her classification systems to quantitatively and qualitatively determine the level of photodamage and prescribe the appropriate chemical peeling combination.
Superficial Chemical Peeling
Superficial chemical peeling is truly an exfoliation of the stratum corneum or the entire epidermis to encourage regrowth, with less photodamage and a more youthful appearance. It usually requires repetitive peeling sessions to obtain maximal results. These agents have been broken down into very superficial chemical peels, which will remove the stratum corneum only, and superficial chemical peels, which will remove stratum corneum and damage the epidermis. It is to be noted that the effects of superficial peeling on photoaging skin are subtle and will not
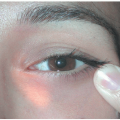
produce a prolonged or very noticeable effect on dermal lesions such as wrinkles and furrows. Agents used include trichloroacetic acid (TCA) 10% to 25%, Jessner solution, glycolic acid 40% to 70%, and salicylic acid (β-hydroxy acid) (
8) (
Table 4.3.4). Each of these agents has its own characteristics and methodology, and a physician must be thoroughly familiar with the chemicals, methods of application, and nature of healing. The usual time for healing ranges from 1 to 4 days, depending on the chemical and its strength.
Very light peeling agents include low concentrations of glycolic acid, 10% TCA, and 20% salicylic acid, which is a β-hydroxy acid. Glycolic acid is an α-hydroxy acid derived from organic products and is pH dependent to produce a superficial chemical peel through keratolysis. Its intensity is dependent on concentration, which ranges from 10% to 70%.
Salicylic acid, called a β-hydroxy acid molecule, is a salicylate derivative in ethanol solution used in concentrations 20% to 40%. Jessner solution is a combination of chemicals: resorcinol, salicylic acid, and lactic acid. It is used as a superficial chemical peel for photoaging skin. Lactic acid is an α-hydroxy acid useful in this combination.
TCA is the most versatile of all peeling agents; its concentration correlates directly with the depth of penetration and thus the degree of destruction within the skin. The concentration usually is compounded in a weight per volume measurement. It is important to distinguish this from the volume per volume formulation because the concentrations do not correlate. Most of the medical literature on TCA peeling uses a weight per volume measurement. TCA usually is standardized as an aqueous solution, although it has been formulated as cream or paste. The author believes there is no distinct advantage to these formulations.
 Preoperative Evaluation of Patients Undergoing Cosmetic Blepharoplasty
Preoperative Evaluation of Patients Undergoing Cosmetic Blepharoplasty
 Fat Repositioning in Transconjunctival Lower Eyelid Blepharoplasty
Fat Repositioning in Transconjunctival Lower Eyelid Blepharoplasty
 Endoscopic Brow Lift
Endoscopic Brow Lift
 The Midface Lift
The Midface Lift
 Hyaluronic Acid and Other Soft Tissue Fillers for Facial Rejuvenation
Hyaluronic Acid and Other Soft Tissue Fillers for Facial Rejuvenation
 Infraorbital Discoloration: Dark Circles—An Anatomic Analysis and Treatment
Infraorbital Discoloration: Dark Circles—An Anatomic Analysis and Treatment



