12. The Medi Spa and Other Practice Considerations
Rishi Jindal, Renato Saltz
PRACTICE BASICS
WHAT IS A MEDI SPA?
■ Fusion of wellness spa, salon, retail store, and medical office practice with or without integrated ambulatory surgery center (ASC)
• ASC defined by Code of Federal Regulations as “any distinct entity that operates exclusively for the purpose of providing surgical services to patients not requiring hospitalization and in which the expected duration of services would not exceed 24 hours following an admission”1
• Definition varies by organization and jurisdiction, but lack of (anticipated) need for overnight admission universal
■ Spa, salon, and retail services offered typically in one part of facility
■ Plastic/aesthetic surgeon functions primarily on medical side in another part of facility
■ Physician on site can allow more advanced “medical spa” services like deep chemical peels, laser therapies, and injectables (see Legal Considerations section).
■ Retail sales of skin care products, camouflage makeup, mechanical or light-based devices (Table 12-1)
Table 12-1 Range of Services Offered in a Comprehensive Medi Spa
| Spa, Salon, and Retail Services | Medi Spa (Noninvasive) Services | Surgical Services |
Chemical peels Facials, skin care, and cosmeceuticals Hand, foot, and nail care Hair care Laser therapies Makeup Massages Scrubs | Deep chemical peels Dermal fillers Intense-pulsed light (IPL) Photorejuvenation Latisse (Allergan) Microdermabrasion Neurotoxin injections Postsurgical skin care | Body Abdominoplasty Body contouring (body lift, brachioplasty, thigh lift) Hand surgery and hand rejuvenation Labiaplasty Liposuction Scar revision Breast (augmentation, reconstruction, reduction) Gynecomastia reduction Mastopexy Facelift Browlift Eyelid surgery Facial implants Hair transplant Otoplasty Rhinoplasty |
TIP: Medi spas can incorporate retail services, salon care, spa services, and noninvasive and surgical cosmetic procedures into one facility; it depends on the surgeon’s interests, goals, and finances.
PRACTICE SETTING
■ Solo practice can offer complete control over all aspects of the practice or medi spa.
■ Conversely, complete responsibility of decisions and finances lies with the physician.
■ Establish who will care for patients, complications, and emergencies when physician is away for personal or professional activities in solo practice.
■ Group practice can offer convenience of trusted colleagues caring for patients.
■ Personal goals, personality, and philosophy are important considerations when deciding to work in a solo or group practice.
■ Hospital-affiliated facility versus truly private practice may affect choice for size of practice, considering “on-call” activities, overhead costs, and ease of becoming established in the specific geographic market.
OFFICE
■ Consider a convenient and accessible location, while maintaining subtlety and privacy.
■ Ensure adequate parking, adherence to all building and city codes, and standards of accrediting organizations.
■ Provide attractive, elegant interior with efficient flow of patients, but avoid gaudy, extravagant, or ostentatious decor and atmosphere.
■ Maintain separation of medical/surgical patients and consumers of retail, salon, and spa services.
STAFF
■ Ensure that all staff knows the practice’s philosophy and embraces it.
■ Ensure the team is trustworthy, knowledgeable, intellectually curious, and dedicated.
■ Hire a business manager, patient coordinator, administrative assistant; expand and focus roles as the practice and business grow.
■ Schedule regular staff meetings.
■ Encourage environment of working hard, generating business, and putting patient safety at the forefront of mission.
■ Maintain professionalism—always lead by example!
TIP: A well-trained, dedicated, trustworthy staff can be one of a physician’s biggest assets in practice. Interview carefully and take the time to hire wisely!
SENIOR AUTHOR TIP: Complete financial and background checks on all potential employees before you hire them.
Embezzlement is a very common problem in medi spa and aesthetic practices. Learn how employees can embezzle and how you can prevent it from happening.
I recommend staff meetings very often, at least on a monthly basis. The focus should be on patient safety, new technology, and proactive staff issues—do not allow drama!
MARKETING AND GETTING ESTABLISHED2
Marketing
■ Telephone is usually the first encounter a patient has with a medi spa, so ensure someone warm and knowledgeable is answering.
■ Have an attractive and informative website; start early, even months before the doors open, and consider a web designer familiar with medi spas.
■ Communications outside the office must have a “call to action”—an intended response, which can be as simple as providing education and contact information to referral sources, potential patients, and community groups.
■ Internal marketing once patients are in the door
• Staff and physician directing communication with patients is the most effective tool.
• Internal branding: Have pamphlets with services you offer, your practice name on pens and mugs, email sign-up list for offers or specials.
• Unique aspect of medi spa is that spa and noninvasive cosmetic procedures can be direct referral into the surgical practice for patients who want to take that step.
• Suggest complementary services, like peels for facelift patients, or offer packages that combine surgical and nonsurgical treatments.
TIP: Physicians should establish a niche, identify a community’s needs or what it lacks in other aesthetic surgeons, and identify why they and their medi spa are unique or novel.
■ External marketing to get patients in the door
• Community outreach: Early in their career or practice, physicians should make themselves available to as many community groups, speaking engagements, and local radio and television shows as possible.
• Meet and engage referral sources by sending educational materials, speaking with other physicians at the local hospital, offering expertise (when it is sought), and later showing sincere gratitude for their support.
Advertising
■ Printed material: Newspaper and magazine advertisements; direct mailings to patients, groups, or referring physicians; pamphlets in the office or handed out at events
■ Electronic material: Email; text messages; radio and television; the website and other Internet sites (Facebook and Twitter)
■ Links from related websites
SENIOR AUTHOR TIP: I recommend having a full-time marketing director and a full-time social media manager. I also recommend a modern, attractive website that needs to be renewed every 2 to 3 years.
SENIOR AUTHOR TIP: Referrals must be carefully studied at minimum every quarter.
FINANCES3
■ Physicians should set goals for themselves and their practice for financial growth, practice expansion, patient management, and experience.
■ Projections can be time consuming, and trying to calculate the cost of goals can be daunting, but goals may go unfulfilled if this is not done.
■ Assets include skills and education, the staff and their knowledge, the patients, and tangibles like products, materials, equipment, and property.
■ Expenses include (1) direct expenses like wages, supplies, cost of operating equipment, and (2) overhead expenses like debt, loans, taxes, monthly bills, equipment rental, and depreciation.
■ Careful planning and some research will allow surgeons to project how to balance their income and assets with expenses and future goals.
■ Determine when taking on partners or nonphysician providers can increase revenue, while not necessarily doubling overhead.
AMBULATORY SURGERY FACILITY CERTIFICATION AND STANDARDS
ACCREDITATION4
■ Before 1980 there were no specific guidelines for ASCs, quality control, or patient safety standards.
■ Plastic surgeons decided to create a certifying body to oversee safe, reliable patient care facilities.
■ They established the American Association for Accreditation of Plastic Surgery Facilities.
■ It was later extended to facilities for all surgical specialties, becoming American Association for Accreditation of Ambulatory Surgery Facilities, Inc. (AAAASF).
■ More than 2000 facilities nationally are AAAASF certified—largest not-for-profit accrediting body of ASCs.
■ In 1996 California was first to mandate AAAASF accreditation for facilities providing sedation or general anesthesia (Legislation AB595).
■ Most State Departments of Health accept accreditation instead of state licensure.
■ AAAASF can also provide Medicare certification.
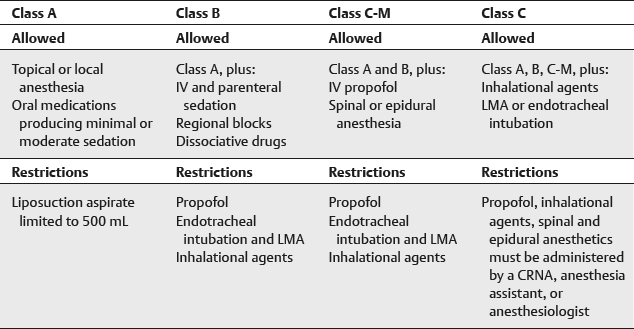
ACCREDITATION OF AMBULATORY SURGERY FACILITY CLASSES5 (Table 12-2)
Table 12-2 Accreditation of Ambulatory Surgery Facility Class Based on Anesthesia


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


