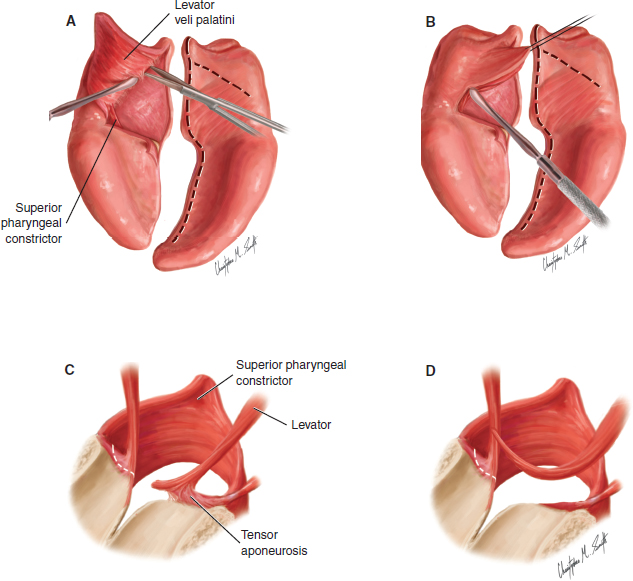
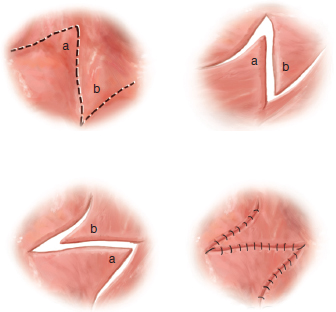
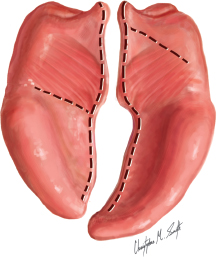
49 ○ Leonard Furlow described the technique of using mirror-image Z-plasties of the oral and nasal surfaces of the velum for cleft palate repair in 1978. ○ The Z-plasty design of the Furlow palatoplasty provides for velar lengthening, prevents velar shortening caused by scar contracture, and allows reorientation of the levator muscle bundles. ○ In the Furlow palatoplasty, the posteriorly based flaps comprise the levator muscles and mucosa; the anteriorly based flaps comprise mucosa alone. ○ The design of the Z-plasty is determined by the underlying palatal anatomy. ○ The levator muscles must be completely released from the posterior edges of the hard palate and from the tensor aponeuroses to allow complete retropositioning of the reconstructed levator sling. ○ Use of lateral relaxing incisions allows tension-free closure of wide clefts and minimizes the risk of oronasal fistula formation. Befere the late eighteenth and early nineteenth centuries, reports are limited of surgical repair of palatal defects, whether congenital or acquired. The primary treatment for patients before cleft palate surgery was a palatal obturator. The role of the palate in the production of speech and the congenital nature of orofacial clefting were poorly understood. The ability to safely perform surgery on the mouth further limited attempts at definitive correction.1 The first published accounts of soft palate repair appeared in 1817 by Carl von Graefe of Germany, followed in 1819 by Philibert Roux of France. These procedures involved cautery of the mucosal margins of the cleft and suturing of the tissues to achieve velar closure.2–4 In the 1820s Johann Dieffenbach of Germany published the first report of hard palate repair by elevation of the hard palate mucosa.5 In 1824 J.C. Warren became the first American surgeon to publish a report of palatal closure after tumor removal, and his son, J.M. Warren, then picked up this torch by performing a series of 24 congenital cleft palate repairs.6,7 Although progress was made with respect to the frequency of cleft surgery, attempts to perfect the surgical technique of palate repair had not yet truly begun. In 1861 German surgeon Bernard von Langenbeck began to advance his techniques of palatal closure and presented major modifications to the original Dieffenbach procedure to close the hard palate. He invented specialized instruments for the procedure, developed the concept of mucoperiosteal flaps, and discussed myotomy to release the levator muscle and relax tension on the mucosal repair. His work forms the basis of modern cleft palate repair, and the techniques based on his work did not change until the early twentieth century.8,9 Over time, it became evident that the classic von Langenbeck repair often resulted in shortening and scarring of the soft palate, leading to poor speech outcomes despite closure of the cleft. Since von Langenbeck, dozens of surgeons worldwide would describe modifications and alternative approaches to closure of the hard and soft palate, each designed to improve outcomes, but a full six decades passed before Victor Veau published any truly new recommendations for the repair of palatal clefts.1 Veau’s theories focused on muscle repair within the soft palate. He promoted Hans Ganzer’s V-Y retropositioning of the hard palate mucosa and described the use of nasal mucoperiosteal flaps and vomer flaps to close the nasal floor and to help prevent deleterious scarring.1,10,11 His revelations and experience influenced surgeons throughout Europe and America. William Wardill and T. Pomfret Kilner, both of England, further advanced Veau’s techniques of V-Y retropositioning of the hard palatal mucosa. Despite clear differences in their surgical approaches (Wardill divided the palatine arteries and performed a simultaneous pharyngoplasty; Kilner did not), the two men are recognized together as innovators of the Wardill-Kilner V-Y pushback, sometimes called the Veau-Wardill-Kilner technique.1,12,13 Although alternative pushback techniques were subsequently described by others, including Dorrance of Philadelphia, the Wardill-Kilner palatoplasty achieved and retained the greatest popularity over the years and remains in frequent use.1,14 In his landmark paper of 1969, Otto Kriens recognized and described the muscular slings of the soft palate and posterior pharynx. He promoted the appropriate reconstruction of these slings and described the first formal intravelar veloplasty (IVVP). He recommended reconstruction of the levator sling and noted the resultant retropositioning.15 This fundamental procedure has been incorporated with some variation into subsequently described repairs. When added to the classic von Langenbeck or Wardill-Kilner approaches, IVVP is widely believed to result in better speech outcomes than do the original procedures alone.16–18 In 1978, at the annual meeting of the Southeastern Society of Plastic Surgeons, Leonard Furlow reported on his new approach to palate repair that included palatal lengthening and reconstruction of the levator sling.19 Apologetically, he noted that his series included only three patients and short-term outcomes. Nonetheless, the method appeared promising, and Peter Randall of the Children’s Hospital of Philadelphia (CHOP) quickly adopted the technique and immediately began to build a large series of his own.1,20,21 The same year, Claus Walter and Hans-Henning Meisel of Germany published a similar double Z-plasty approach designed to lengthen the palate and to reorient the muscles.22 This procedure focused on leaving the muscle fibers attached to the oral and nasal mucosal flaps rather than performing a complete muscle dissection, as in the classic IVVP. Unlike Furlow’s procedure, however, theirs did not specifically separate the fibers into the posteriorly based flaps, but rather split the fibers randomly so that some would, by nature of the technique, become severed from their direct neurovascular supply and remain in the wrong position. Although some fibers would become appropriately repositioned, the rest would be inappropriately positioned or lost altogether. This could result in decreased muscle bulk with hampered ability to adequately elevate the palate because of muscle weakness or inappropriate vector of pull. Walter and Meisel reported good healing and normal palatal movement but did not report on their speech outcomes.1,18,22 It wasn’t until several years later that published accounts of the Furlow technique became available, the first a series of 106 patients by Randall in April 1986, followed by a series of 22 patients published by Furlow in December 1986.18,20 Furlow’s description of “cleft palate repair by double opposing Z-plasty” is now simply referred to primarily as the Furlow palatoplasty.18 The published technique used the concept of Kriens’ muscle sling reconstruction and focused on changes in the approach to repair the soft palatal cleft. Furlow described improved positioning of the soft palate musculature and velar lengthening through the use of mirror-image Z-plasties of the oral and nasal surfaces, while sparing pushback or complete elevation of the hard palate to avoid scarring and subsequent midfacial growth disturbance. In his initial published report, he provided speech follow-up for 20 of the 22 patients, noting that 18 had normal resonance and 2 had evidence of only mild velopharyngeal dysfunction.18,20 Cleft palate repair has long been understood to be necessary for the development of normal speech and resonance, but the optimal design, timing, execution, and reproduction of this surgical challenge has eluded many. The modern goals of palatoplasty for congenital or acquired palatal defects include the separation of the oral and nasal cavities at the level of the alveolus, hard palate, and velum to allow functional uncoupling of the oral and nasal cavities for feeding and speech. This includes reconstruction of the musculature of the soft palate into a more normal anatomic position in relation to each other and to the posterior and lateral pharyngeal walls. Although congenital palatal defects invariably involve some degree of soft tissue deficit, repair techniques should aim to provide adequate closure at the primary setting rather than rely on secondary or revisional surgery amidst scar and soft tissue contraction to achieve complete closure. Meticulous surgical planning and technique is necessary to prevent postoperative oronasal fistula formation, which may necessitate more challenging subsequent corrective procedures. Maintenance of midfacial growth and determination of optimal surgical timing for normal speech development provide additional challenges to the execution of the perfect palate repair. The Furlow palatoplasty successfully addresses most, if not all, of these goals, because it focuses on a safe, reliable closure with a decreased risk of oronasal fistulas, functional muscle repositioning, lengthening of the soft palate, and limited postoperative velar shortening. Superior speech results have been reported by many authors that have adopted the technique since its original description.23–30 The somewhat more limited data on midfacial growth after Furlow palatoplasty is also encouraging.31 Fig. 49-1 Standard Z-plasty design. The concept of the Z-plasty in plastic surgery is certainly not new, although its origins have been debated. The first report of a Z-plasty, although not named as such, is believed to be that of Charles Denonvilliers of Paris in the mid-nineteenth century.32 In 1968 David Furnas33 described the four fundamental functions of the Z-plasty as being (1) to increase length, (2) to break up a straight line, (3) to shift topographic features from one site to another, and (4) to efface or to create a web or a cleft. The Furlow palatoplasty employs the first three functions to significant benefit. The basic Z-plasty design is that of two independent triangular flaps made along a shared straight line, with their positions then swapped to reorient the flaps in a horizontal, interlocking fashion (Fig. 49-1). This repositioning redirects the tissues and healing vectors and secondarily adds length to the incision. Incisional reorientation adds the benefit of disruption of the straight-line scar, which can otherwise shorten over time from scar contraction. Although the individually shorter limb lengths of the incision can shorten, overall shortening is less than that for a single straight line scar of the same length. Furlow’s original design of the double-opposing Z-palatoplasty uses mirror-image Z-plasty patterns on the oral and nasal surfaces to close the tissues of the soft palate. The posteriorly based flaps on both surfaces comprise both muscle and mucosa, whereas the anteriorly based flaps contain mucosa alone. On the oral surface, the design is typically marked with the posteriorly based flap on the left side of the palate and the anteriorly based flap on the right. In fact, the posteriorly based oral myomucosal flap may be designed on either side of the cleft, but its elevation by a right-handed surgeon is made easier when the flap is designed on the patient’s left side. Fig. 49-2 Design of the oral incisions. The lateral limb for the posteriorly based myomucosal flap extends from the cleft margin at the hard palate–soft palate junction to the region of the hamulus; the lateral limb for the anteriorly based flap extends from the cleft margin at the base of the uvula to the region of the contralateral hamulus. However, the Z-plasty design must always be based on the underlying anatomic landmarks and not on any predetermined linear or angular measurements. Hence the angles of the Z-plasty design on either side of the cleft may differ in asymmetrical clefts. The central limb of the design is first placed along the cleft margin on each side of the cleft. The anterior incision for the posteriorly based oral myomucosal flap is then drawn along a line that extends from the hamulus, along the posterior edge of the hard palate, and to the cleft margin. This limb must continue as a straight line along the vector of the posterior hard palate and not curve anteriorly to follow the margin of the underlying bony cleft. The posterior incision of the contralateral oral mucosal flap is then drawn from the base of the uvula to the hamulus on the corresponding side. Following elevation of the flaps on the oral surface of the soft palate, the “opposing” Z-plasty is created on the nasal surface as a mirror image of that on the oral side. Thus the posteriorly based nasal myomucosal flap is created on the side of the anteriorly based mucosal flap by designing a nasal mucosal incision that extends from the cleft margin to the region of the hamulus, and the anteriorly based nasal mucosal flap is created on the contralateral side by designing a nasal mucosal incision that extends from the base of the uvula to the region of the hamulus (Fig. 49-2). The design of opposing Z-plasties allows complete palatal closure, lengthening of the velum, and repositioning of the levator muscles, all while providing well-vascularized flaps that will be sutured without overlapping incisions, thereby helping to prevent a postoperative fistula. On the oral side, the posteriorly based flap is typically designed on the left side of the soft palate. As noted previously, the anterior limb of the Z-plasty is designed along a diagonal from the hamulus to the cleft margin along the posterior edge of the hard palate. This most often creates an angle with the central limb that approximates 60 degrees. The anteriorly based flap is typically designed on the right side of the soft palate. The posterior limb of the Z-plasty is placed along a diagonal from the base of the right-sided uvula toward the ipsilateral hamulus, most often creating an angle with the central limb that measures 60 to 80 degrees, depending on the length of the velum. Before it is dissected, the soft palate is infiltrated with a diluted epinephrine-containing solution to provide hemostasis. The posteriorly based flap is incised and elevated with oral mucosa and levator muscle as a composite myomucosal flap. The abnormal levator attachments to the posterior edge of the hard palate are carefully divided as the flap is elevated from medial to lateral. The myomucosal flap is lifted and dissected posterolaterally, with the levator muscle bundle carefully separated from the underlying nasal mucosa with scissors (Fig. 49-3, A). In the appropriate plane, this is typically a hemostatic dissection, and care should be taken to avoid perforating the underlying nasal mucosa. A Freer elevator can be used to help bluntly separate the muscle from the underlying nasal mucosa and from the transverse fibers of the superior pharyngeal constrictor laterally (Fig. 49-3, B). Completely separating the levator muscle from the tensor aponeurosis near the hamulus is critical to allow complete posterior rotation of the myomucosal flap and placement of the levator muscle fibers into the correct position (Fig. 49-3, C and D). On the right side of the soft palate, the mucosal flap is incised and elevated starting at the base of the uvula, with the mucosa carefully elevated off the underlying muscle. Thedissection is carried anteriorly to the posterior edge of the hard palate, remaining in a plane deep to the submucosal glands (Fig. 49-3, E). This dissection must be performed with great care to avoid tearing or perforating the oral mucosa, particularly at the base of the flap where the mucoperiosteum is usually quite adherent to the underlying palatine bone.
The Furlow Double-Opposing Z-Plasty Repair for Cleft Palate
Alison Kaye, Richard E. Kirschner
KEY POINTS
LEONARD FURLOW AND THE DOUBLE-OPPOSING Z-PLASTY
Goals of Palatoplasty
ANATOMY AND OPERATIVE DESIGN
Brief Review of the Z-Plasty Concept
Soft Palate Landmarks and Incision Design
Elevation of the Flaps: Oral Surface
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine