Reconstruction of the Cleft Maxilla and Alveolus
Bernard J. Costello, Ramon L. Ruiz
KEY POINTS
○ An interesting aspect of the development of cleft care has been the reconstructive options of the alveolar and maxillary defects, because the outcome data in this area have helped shape the general approaches to cleft care worldwide as a balance between aesthetic, functional, and growth concerns.
○ The specific timing of alveolar cleft grafting is a controversial area, and several prevailing opinions may be considered.
○ The techniques used for the reconstruction of alveolar and maxillary defects must be aimed at the primary objectives of the procedure, and not simply at providing bone to the alveolar ridge.
○ Phase I orthodontic expansion is necessary for most cases involving palatal clefting behind the incisive foramen to align the arches before grafting.
○ The ideal standard for reconstruction of the cleft maxilla is autologous bone from the anterior iliac crest.
○ Most patients have minor discomfort associated with iliac crest bone grafting and benefit from a local injection of a low dose of bupivacaine at the end of the procedure for long-lasting anesthesia during the initial recovery period.
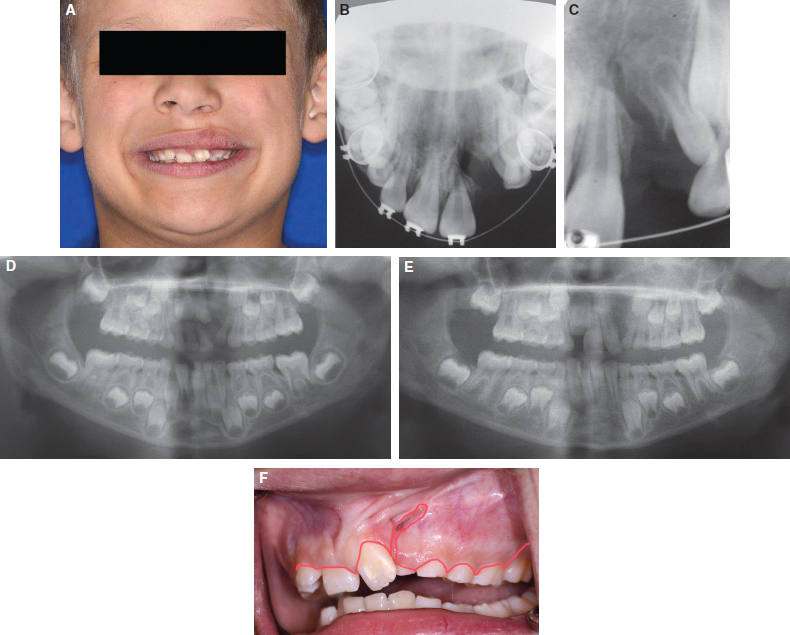
Clefting of the maxilla and alveolus results from a failure of fusion of several key components of the facial structures during the first trimester and typically includes components of the maxillary processes, median nasal process, and palatal shelves.1 When one or several of these components fail to fuse, a variety of clefts can be seen. Each bone and soft tissue defect is reconstructed in a particular fashion and is staged based on growth, functional needs, and aesthetic concerns. Despite successful lip repair and closure of the hard and soft palate during infancy, a residual nasolabial fistula and bony cleft defect that involves the alveolar ridge, maxilla, and piriform rim will remain.2,3 These residual deformities are most often addressed by secondary bone grafting performed during the mixed dentition stage of middle childhood (6 to 10 years of age).2,3 The objectives of bone graft reconstruction of the cleft maxilla are to establish adequate bony matrix for eruption of the permanent cuspid tooth, to close any residual alveolar oronasal communication, to establish continuity of the maxillary ridge, and to improve the underlying support of the nasal base (Fig. 69-1). In the case of bilateral cleft lip and palate, an added benefit of bone graft reconstruction is stabilization of a mobile premaxillary segment.
Approximately 75% of patients with orofacial clefting require reconstruction of the maxilla and alveolus.2–4 The timing of this procedure should be based on dental development and not on chronologic age. Bone graft reconstruction of the cleft site is typically performed during mixed dentition, just before eruption of the permanent canine or the permanent lateral incisor. However, some controversy exists regarding the timing of this reconstruction. On the basis of work performed by Boyne and Sands,4 most surgeons reconstruct this area during mixed dentition before eruption of the permanent canine. Earlier reconstruction of this area has been associated with a high degree of maxillary growth restriction, necessitating orthognathic surgery later in life in a much higher percentage of patients.2,4–9
Fig. 69-1 This child with a left unilateral cleft of the lip and palate exhibits the typical depressed piriform rim and maxilla in the area of the bony cleft. Although rhinoplasty can be used in an attempt to provide symmetry to the nose, the primary lack of structure is associated with the maxillary and alveolar cleft. The defect in the bone at the alveolar level may be fairly small, but attention is required at the remainder of the maxilla to provide an adequate reconstruction to achieve all of the goals. Note the proximity of the central incisor to the cleft.
The ideal timing, technique, and reconstructive materials are matters of great controversy. This chapter reviews those associated with secondary reconstruction of the cleft alveolus and maxilla. Primary reconstruction, gingivoperiosteoplasty, and late secondary reconstruction are discussed more comprehensively elsewhere in this text.
HISTORY
An interesting aspect of the development of cleft care has been the reconstructive options of the alveolar and maxillary defects, because the outcome data in this area have helped shape the general approaches to cleft care worldwide as a balance between aesthetic, functional, and growth concerns. The differing opinions in the literature highlight the progression of the techniques involved in the long-term care of children with clefts and the current focus on long-term outcome and growth as a key factor of those outcomes.
In the 1950s, the concept of primary or early bone grafting of the cleft maxillary defect was introduced by Schmid.10 Although the concept was initially met with enthusiasm from a number of surgeons, primary bone grafting eventually was abandoned because of unfavorable outcomes. During the decades that followed, the negative skeletal, dental, and growth-related consequences of primary bone grafting became better understood.2,5,6 During the early 1970s, Phillip Boyne4 was the first to publish favorable outcomes using autologous particulate bone grafts for reconstruction of the cleft maxilla and alveolus later in childhood during mixed dentition rather than earlier in life. Although Boyne’s work and results represented a landmark discovery in the field of cleft reconstruction, cleft palate teams were slow to integrate the approach into their treatment protocols because of the negative associations that lingered after the poor outcome experience with primary bone grafting. Today, Boyne’s principles of secondary bone grafting represent the standard approach for most of the world’s cleft centers.2–4 Debate continues regarding the preferred protocols for reconstructing this area, and the approaches taken offer considerable nuance.
Debate regarding primary gingivoperiosteoplasty, its success, and its consequences on growth have reignited these discussions.11–15 These early studies and experiences have set the stage for evaluating improvements in the long-term outcome for patients with clefts and for careful considerations of the burden of care on patients, parents, and health care delivery systems in light of those outcomes.9,13
TIMING OF REPAIR
The specific timing of alveolar cleft grafting is a controversial area, and several prevailing opinions may be considered. For the purposes of comparative discussion, the major options are briefly discussed here. The common options include gingivoperiosteoplasty, primary bone grafting, and secondary bone grafting.
Gingivoperiosteoplasty is performed in infancy, typically at the time of cleft lip repair. Some clinicians believe that performing a procedure during the lip repair to bridge the gap across the alveolar defect with small periosteal flaps can produce bone union between the segments, thus potentially preventing the need for bone grafting later in life.9 Although some results have been favorable, the published results are mixed with respect to amount and quality of bone to be provided at the cleft site for eruption of the permanent dentition (i.e., the canine and lateral incisor).11 A significant percentage of patients will still require grafting at a later date before the eruption of the permanent teeth because of insufficient bone volume. Significant growth restriction and maxillary hypoplasia have been observed with this technique, although it is still common in many centers. Several reports have confirmed this concern whether the reconstruction is performed in the standard fashion or with the addition of bone or bone morphogenetic protein (BMP).15
Primary bone grafting is typically performed in early childhood. Primary bone grafting in the young child was the first attempted protocol to use bone (rib) to reconstruct the alveolar cleft and was widely used in the 1960s.2–4,10,16–22 Growth restriction was present in most patients, and as a result, this timing protocol has been discarded by most centers worldwide.5–7 A few centers still use this protocol and have published good results.22 However, recent studies have questioned these positive growth results.
Secondary bone grafting before the eruption of the relevant permanent dentition remains the most commonly performed protocol.2–4,9 Procuring bone graft from the iliac crest, cranium, mandibular symphysis, or other locations has been the standard for reconstruction of this site since Boyne’s initial descriptions. Several key factors determine the ideal time for grafting, and they include a number of anatomic and growth variables. Typically, the timing is based on root formation of the permanent canine based on radiographs, with grafting performed when the root is one-half to two-thirds formed. Should a lateral incisor be present and of good morphology, then the surgeon may consider performing earlier secondary bone grafting to the maxilla and alveolus. Grafting may then be performed slightly earlier, when at least half of the lateral incisor root is present. The lateral incisor erupts earlier than the canine, and if it erupts early into the ungrafted cleft site, periodontal health may be compromised.
Another important timing factor is the ability to perform phase I orthodontic expansion of the maxilla using a quad-helix or similar appliance before grafting. Some prefer to wait for eruption of the permanent maxillary first molars to provide anchorage for the orthodontic expander rather than using the primary teeth for anchorage or a soft tissue–based appliance. Appliances that provide force directly using the palatal shelves may affect the blood supply of the flaps used during the surgery and create a significant hygiene problem by causing inflammation of the flaps typically used for closure. Given all of these factors, the repair typically occurs during the 6- to 10-year age range, but timing is determined based on dental development rather than on chronological age.
In addition, if the central incisor is bordering the cleft, some consideration can be given to earlier-than-typical grafting to provide adequate periodontal support to this area (see Fig. 69-1). Some literature supports this technique, because the periodontal outcomes have been reported to be improved. No randomized or controlled studies, however, have shown this to be an improved protocol in a comparative fashion. As with gingivoperiosteoplasty, bone retention and bone heights have been shown to be quite good in the initial reports from those who favor this approach, but the comparative studies using this protocol are still lacking.
PRESURGICAL ORTHODONTIC CONSIDERATIONS
Phase I orthodontic expansion is necessary in most cases involving palatal clefting behind the incisive foramen to align the arches before grafting. Expanding after grafting typically does not work as effectively because of the lack of a palatal suture and the subsequent challenges in controlling the transverse dimension orthodontically. Bone grafting effectively solidifies the transverse dimension; thus preoperative expansion becomes very important to help optimize the chances for arch compatibility at skeletal maturity. This minimizes the chance for crossbites and the need for segmental osteotomies of the maxilla, which can be particularly unstable in this group because of palatal scarring, later in life. Having the transverse dimension expanded appropriately is a major goal of this phase of therapy.
A common mistake to avoid is that of failing to expand the maxilla completely before grafting, with the theoretical concern that the cleft would be too large for the surgeon to close. Typically, mobilizing the various flaps involved and closing the nasal mucosa with maximal expansion is much easier. Minimal anterior expansion can make it difficult to place sutures in the nasal mucosa in certain clefts. Therefore maximal preoperative expansion is recommended and actually improves the ability for the surgeon to mobilize nasal flaps for closure. Oral-side flaps are typically not difficult to mobilize, even in large defects.
Bilateral clefts may require additional phase I orthodontic expertise, because the premaxillary segment is typically protrusive and often asymmetric relative to the other components of the maxilla and to the mandible. Taking the premaxillary segment out of occlusion with the lower arch using presurgical phase I orthodontic and orthopedic techniques is important to avoid motion of this segment after grafting. Motion of the premaxillary segment while under function after grafting often causes a nonunion of the segments. A palatal splint is placed after the graft is completed and may be used to minimize force on the anterior segment and to protect the graft from occlusal trauma.
If primary, supernumerary, or nonrestorable teeth are present in the cleft site, then a consideration should be made for presurgical extraction, allowing healing time before the definitive bone grafting procedure. Alternatively, teeth can be removed at the time of grafting, but for clefts that may be difficult to close, there is an advantage to allowing secondary intention healing to occur at the extraction sockets for additional gingiva to be used during the repair.
SURGICAL TECHNIQUES
The techniques used for the reconstruction of alveolar and maxillary defects must be aimed at the primary objectives of the procedure, and not simply at providing bone to the alveolar ridge. Despite successful lip repair and closure of the hard and soft palate during infancy, a residual nasolabial cleft that involves the alveolar ridge, maxilla, and piriform rim will remain. The objectives of bone graft reconstruction of the cleft maxilla are to establish adequate bony matrix for eruption of the permanent cuspid tooth, to close any residual alveolar oronasal fistulas, to establish bony continuity of the maxillary ridge, and to improve the underlying bony support of the nasal base. In the case of bilateral cleft lip and palate, an added benefit of bone graft reconstruction is stabilization of a mobile premaxillary segment.
The techniques can be separated for discussion based on whether they involve limited advancement flaps, broad advancement flaps, or mucosal pedicle flaps to rotate into larger defects with subsequent gingival reconstruction. The techniques can also be discussed in terms of unilateral or bilateral cleft types. In general, reconstruction of the maxilla and alveolus is performed in one step, whether the cleft is unilateral or bilateral. The defect in bilateral clefts is continuous from side to side, so the concept of repairing one side at a time, in a staged fashion, is anatomically misguided. Often, the septum is undescended superiorly, and no clear division is present from side to side in the area of the incisive foramen.
Unilateral Maxillary and Alveolar Cleft Reconstruction
Broad advancement flap techniques are often used to close small and large defects in the alveolus and maxilla. These techniques involve making crestal incisions along the gingival crevices with posterior releases that are low and allow sliding advancement of the gingival flaps toward the defect (Fig. 69-2). The residual unrepaired cleft is dissected, completely separating the nasal mucosa from the oral mucosa and separating the flaps with enough space superiorly to allow for bone grafting. Experienced surgeons will recognize that a well-repaired nasal floor from the primary lip and nose reconstruction is quite helpful in facilitating this dissection during the bone grafting stage. When only one stitch is placed at the nasal sill during the primary closure, it can be difficult to subsequently dissect two distinct flaps of oral mucosa and nasal mucosa with adequate space at the piriform rim for bony reconstruction.