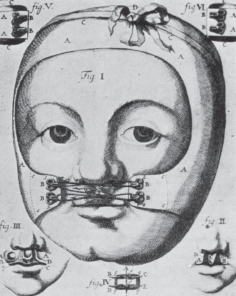
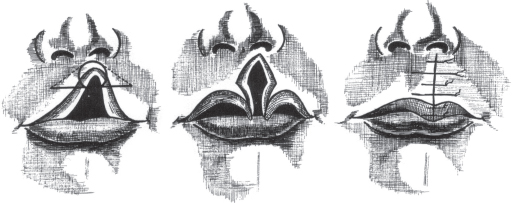
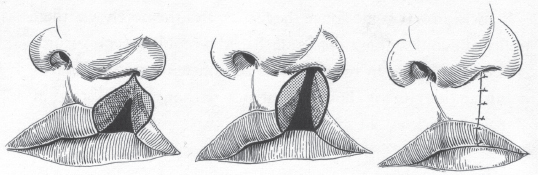
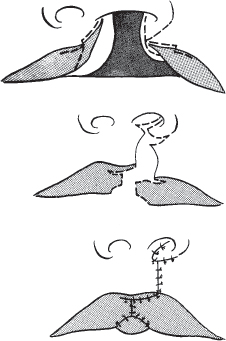
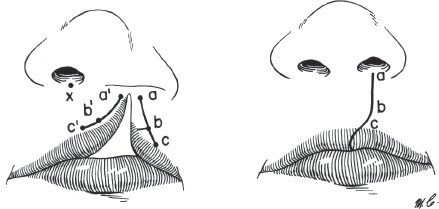
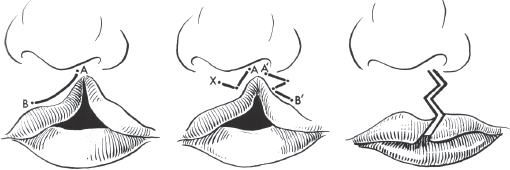
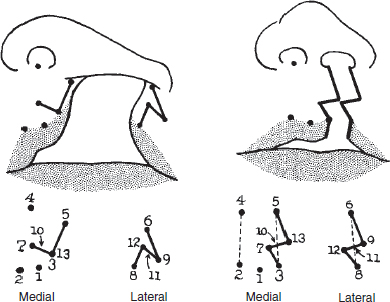
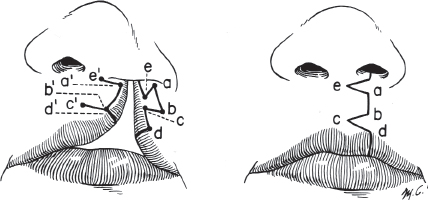
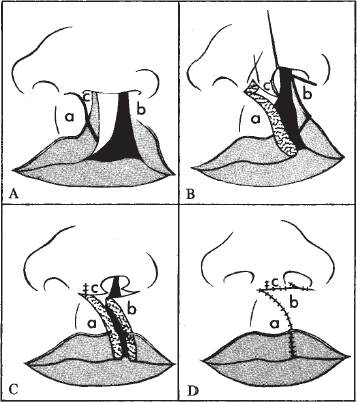
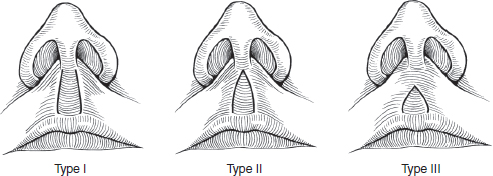
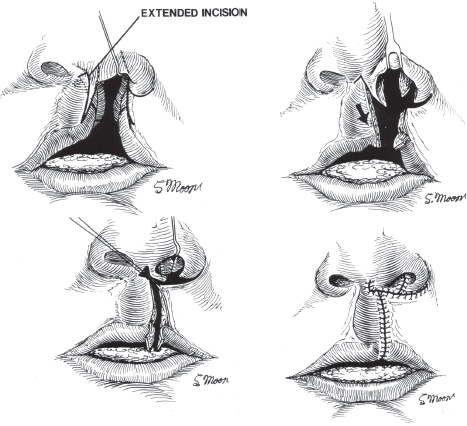
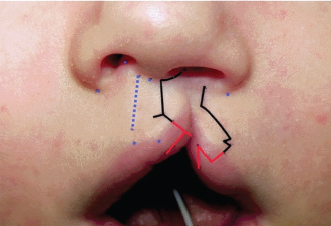
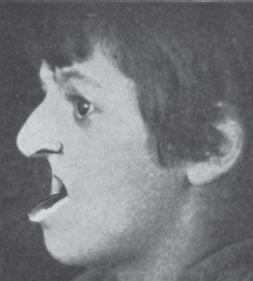
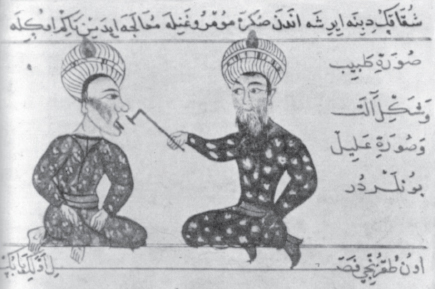
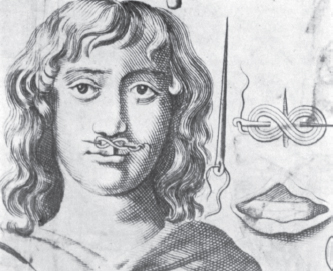
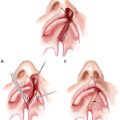
39 ○ The oldest representations of cleft lip come from 3000-year-old mummy grave pottery (huacos) from ancient Peru. ○ The first detailed report of a successful cleft lip repair is from 390 AD from the end of the eastern Chin Dynasty of ancient China. ○ Surgery for cleft palate lagged far behind surgery for cleft lip because of inadequate anesthesia as well as the belief that clefts of the palate were caused by infection with syphilis. ○ Pierre Franco (1505-1579) was likely the first to describe the congenital origin of cleft palate and was one of the first to recognize the importance of the palate for speech. ○ In 1816 in Berlin, Carl Ferdinand Graefe, followed shortly after in 1819 in Paris by Philibert-Joseph Roux, published the first successful cleft palate repairs. ○ The advent of chloroform anesthesia, after its first use in 1847, allowed rapid progress in cleft surgery. Although cleft lip and palate occur throughout the world today, there are few reports from ancient cultures.1 Some of the oldest representations of cleft lip are found in the 3000-year-old “huacos,” or mummy-grave potteries, from Peru2 (Fig. 39-1). The mysterious female figure shown here has an obvious unilateral cleft lip, but unbelievable symmetry of the nose. The ancient Egyptians wrote about the medical and surgical care of facial trauma (including the use of pressure dressings), but they did not mention clefts or their care.3 In The Operative Story of Cleft Palate, George Dorrance reports that an Egyptian mummy was discovered with a cleft palate.4 Also, a dental prosthesis made of gold wiring and fixed to the teeth was found in El Gizeh dated approximately 2500 BC, representing the first known intraoral prosthesis.7 Clefts are scarcely mentioned in the writings from ancient Greece and Rome. They do not appear in the writings of Hippocrates (460-375 BC) or of Celsus (25 BC to 50 AD), best known for his medical encyclopedia De Medicina. Perhaps the first mention of a cleft in ancient European history is in the writings of the physician Galen (131-206 AD), wherein he refers to clefts of the lip as colobomatae.4 Galen is also credited with first using the word lagocheilos, or “lip like a hare.”8 According to some reports, prosthetic obturation of palatal clefts was used commonly in the ancient Roman world during the time of Celsus.7 In his writings from about the sixth century BC, Sushruta, the great surgeon of ancient India, describes a number of surgical procedures involving the lips and face, but it is unclear whether any of these were for congenital clefts. He describes procedures on the uvula: “… by means of forceps between thumb and finger, drawing the uvula forward, the physician may cut it with a sickle-shaped knife above the top of the tongue.”9 The written history of ancient China is more illustrative. A translation by Boo-Chai9 of an ancient Chinese text reveals many written accounts of cleft lip repairs and cleft lip surgeons: “In the Chin Dynasty (229-317 AD), there was a surgeon who did plastic surgery for harelip. In the Tang Dynasty (618-901 AD) another surgeon, Fang Kan, was designated as ‘the doctor of lip repair’ from which he obtained ‘considerable repute’.” The story of the first well-described cleft lip repair, also retold by Boo-Chai,9 dates back to 390 AD and comes from the text of the Chin Annals, an official history of the Chin Dynasty commissioned by Emperor Tang Tai-Tsung (627-650 AD). The patient, Wei Yang-Chi, also called Chang Tao, was from a poor family of farmers from the city of Jen, and at age 18 years presented himself to the Governor of the State of Chu seeking a cure for his deformity. The governor’s surgeon agreed to repair the cleft, but with strict conditions after surgery: “I can cure your condition by cutting and stitching the edges together. However, after the operation it will be necessary for you to rest the affected part for 100 days. During this time you can ingest only thin gruel and you cannot smile or talk.” The story has an interesting ending: “This young man overcame his handicap and became Governor General of six Chinese provinces. This resulted in the perception, which persists in some South Sea Island countries even today, that those with clefts are special and have been touched by God.”10 In Turkey, Charaf ed-Din authored the first Turkish surgical manuscript (ca. 1465) and carried on the traditions of the great Arabian surgeon Albucasis (936-1013 AD) of Cordoba, Spain. In his illustrated manuscript is an image depicting the cauterization of a lip fissure with a hot iron; this technique is believed by some to be used by Turkish surgeons for clefts of the lip as well (Fig. 39-2). The edges of a cleft lip were touched by a very hot iron, thus creating a third-degree burn. After separation of the eschar, the edges were sutured together to repair the cleft. This technique circumvented the need to make an incision and, what is more important, the need to control blood loss.11,12 Surgical progress was slow in Europe because of the prevalence of postoperative infections, inadequate anesthesia, and the inability to control bleeding. The first description of a surgical cleft lip repair did not appear until approximately 950 AD in a book entitled The Leech Book of Bald from pre-Norman Britain.1 Saxon surgeons at that time were known as “leeches.”13 In this manuscript, it is written: “… fore harelip, pound mastic very small, add white of egg, and mingle as thou dost vermilion, cut with a knife the false edges of the lip, sew with silk, then smear without and within with the salve, ere the silk rot.”14 Numerous descriptions of cleft lip repairs are found in European literature from the thirteeth to seventeenth centuries, all of which fundamentally comprise freshening of the cleft edges and suturing them together with the adjunct of various dressings and salves to promote healing and combat infection. For example, the Flemish surgeon Jehman Yperman (1295-1351) wrote that unilateral and bilateral clefts may be “sutured with needles some distance from the cut margins and wrap around with figure eight.”14 He noted that some surgeons used relaxing incisions externally and laterally in the cheek, but advised against their use, because the subsequent facial disfigurement might “compromise the reputation of the surgeon.” In France, Ambroise Paré (1510-1590), one of the great surgical figures of the Renaissance, and his student Guillemean used silver needles with tips of steel and thread of waxed linen. In 1575, Paré popularized the term bec-de-lieure, or “lip of hare,” to describe a cleft lip. He was likely the first surgeon to include an illustration of the repaired lip in his surgical works15–18 (Fig. 39-3). Fig. 39-4 Johan Philip Hofmann of Heidelberg in 1686 described this snug cloth cap that extended over the cheeks and upper lip with hooks and threads to pull the edges of a cleft lip closer together. Another famous Renaissance surgeon, Gaspar Tagliacozzi (1545-1599) of Bologna, Italy, described his repair in 1597. He used a sharp knife or scissors, and he stressed the importance of full-thickness sutures through the lip. In his writings, Tagliacozzi noted that “the Artist must therefore pass his Needle straight through the Lip from the outside inwards, and on the other side, he must pass the Needle from the inside outwards.” He also recommended “some compresses, dipped in Whites of Eggs and Rosewater … applied both to the inside and the outside of the Wound.”1,19 In addition to the various ointments and salves used to promote healing, compression bandages commonly were applied during surgery to assist in closure. Fabricius of Aquapendente20 (1537-1619), a famous anatomist, physiologist, and surgeon who practiced primarily in Padua, Italy, described in 1619 how, in wide clefts, he used an “agglutinative Bandage” to bring the edges of the cleft together or to relieve tension on the cleft margins before he started to freshen the edges. In 1686 Johan Philip Hofmann21 of Heidelberg described a snugly fitting cloth cap with extensions over the cheeks and upper lip. These extensions had hooks around which he would wind thread to pull the edges of the cleft closer together (Fig. 39-4). Other notable cleft surgeons in early European history were Van Roonhuyse22 (1622-1672), a surgeon from Amsterdam, who was one of the first to recommend surgery for cleft lip in patients as young as 3 to 4 months, and James Cooke (1614-1688), an English surgeon from Warwick. Cooke23 advised the following perioperative regimen when operating on such a young child: “If possible (the infant should be) kept from sleep for ten or twelve hours before the operation, that it may be disposed to sleep presently after. For it have ready a glass of wine or cordial, in case of fainting upon loss of blood. Observe, if there be great deformity, what to do, lest you make it worse than it was.” Straight-line closures of clefts of the lip remained the standard approach for the early part of the nineteenth century. Two French surgeons, Joseph Malgaigne and Germanicus Mirault, dissatisfied with the inevitable postoperative contracture of the straight-line lip repair and resulting “whistling” deformity, were among the first to develop alternative repairs. In 1843 Malgaigne described a two-flap operation to lengthen the lip.6 He turned down flaps of skin from each side of the cleft and made horizontal full-thickness cuts on either side of the cleft, which he opened and sutured to each other, lengthening the lip (Fig. 39-5). In 1844 Mirault further refined this technique, resecting the turned-down medial flap, making only one horizontal incision on the lateral lip and bringing the resulting triangular flap of lateral skin and vermilion across medially6 (Fig. 39-6). He thus attempted to fill out the vermilion in the line of the incision to avoid the notch deformity. Mirault described many variations of this closure with different flaps from both sides of the cleft; however, he is remembered best for his innovative triangular flap, which has remained in the cleft surgeon’s armamentarium in one form or another for more than 100 years. In the second half of the nineteenth century, M.H. Collins of Dublin contributed significantly to cleft lip repair by addressing the displaced alar base.6 He designed a small laterally based flap at the alar base and inserted this into a small incision made in the base of the columella. He anchored this flap into the periosteum of the nasal spine. This technique improved alar base symmetry, built a firm nasal floor, and filled out a small “shoulder” in the base of the columella to restore a more normal contour. Fig. 39-5 The Malgaigne two-flap operation designed to lengthen the lip and rebuild the “tubercle.” Fig. 39-6 Mirault’s operation made only one horizontal incision on the lateral lip, thus creating a triangular flap of skin and vermilion that was advanced medially. Fig. 39-7 The incisions for unilateral cleft lip repair designed by William Rose in 1879, which curved away from the center of the cleft to lengthen the closure. In 1879 William Rose proposed curving the incisions away from the center of the cleft to lengthen the closure6 (Fig. 39-7). In 1912 James Thompson, professor of surgery at the University of Texas in Galveston, further refined this technique by paring the cleft edges in the shape of a diamond excision and advocating the use of a compass to mark the angled incisions so that they would be precisely matched. This technique of curved incisions became known as the Rose-Thompson repair. Although Rose and Thompson are given credit for this design, Von Graefe in 1816 and Husson of Great Britain in 1836 both had previously suggested similar curved incisions in their lip repairs.6 Victor Veau of Paris (Fig. 39-8) was widely admired in the field of cleft surgery. In 1925 he published a technique for unilateral repair similar to Mirault’s final design; however, he quickly abandoned this technique for a more complex variation that was intended to lengthen the cleft margins by paring and repositioning the alar base.6,24 He discarded a minimum of tissue and focused on a good muscular approximation with suture, known as his suture musculaire. In addition to repositioning the alar base, he also closed the nostril floor and the anterior palatal cleft along with the cleft lip (Fig. 39-9). He was criticized by some for the asymmetry of the Cupid’s bow produced by his repair. Because Veau was such a prominent surgeon in the field of clefts, however, his design was embraced by many, and he had a significant influence on cleft surgery in Europe.6 At the same time, Vilroy P. Blair and James Barrett Brown also were experimenting with and perfecting Mirault’s original technique in the United States. They were both general surgeons at Washington University in St. Louis, and they dominated the cleft lip surgical scene in the United States in the 1930s and 1940s. Blair is remembered for heading the Head and Neck Team at the Walter Reed Army Hospital in Washington, DC, during World War I, and, with Dr. Robert Ivy, for forming and instructing teams sent to France to treat the many head and neck injuries resulting from trench warfare. He started the plastic surgery programs at Barnes Hospital and the St. Louis Children’s Hospital at Washington University. Barrett Brown joined Blair in St. Louis in 1923, and together in 1930 they published “Mirault’s Operation for Single Harelip.”25 Fig. 39-8 Veau designed a unilateral cleft lip operation to lengthen the cleft margins by paring and repositioning the alar base. Fig. 39-9 The Blair-Brown-Mirault operation, designed by Vilroy Blair and James Barrett Brown in the 1920s and similar to Mirault’s original triangular flap design. The operation described by Blair and Barrett Brown employed a small triangular flap from the lateral side of the cleft above the vermilion to add length to the incision and fullness to the lower part of the lip (Fig. 39-10). They were also among the first to try to correct the cleft nostril width and flattened nasal tip. Later, Barrett Brown with Frank McDowell, another respected St. Louis surgeon, added measurements related to specific anatomic landmarks so that reliable reproducible results could be obtained and tailored to each child.26 This Mirault-Blair-Brown-McDowell method became very popular because it achieved good symmetry and excellent nasal correction. It resulted, however, in a high point of the vermilion in the center of the lip and little semblance of a Cupid’s bow. Moreover, it did not address the maloriented cleft orbicularis muscle.27 At one point, the Mirault-Blair-Brown-McDowell method was likely the most popular operation for unilateral cleft lip in the United States, although some surgeons, including Professor Kilner of Oxford, still preferred the straight-line closure method.28 Fig. 39-10 The Blair-Brown-Mirault operation, designed by Vilroy Blair and James Barrett Brown in the 1920s and similar to Mirault’s original triangular flap design. Fig. 39-11 Le Mesurier’s quadrilateral flap operation put a curve in the vermilion on the cleft side to create a Cupid’s bow. The next milestone in cleft lip repair was to create a Cupid’s bow, and Le Mesurier of the Hospital for Sick Children in Toronto is credited with accomplishing this. He designed a quadrilateral flap from the lateral aspect of the lip, which put a curve in the vermilion on the cleft side to mimic the Cupid’s bow on the noncleft side30,31 (Fig. 39-11). Le Mesurier admitted his design was not original, but similar to the flap described by the German surgeon Hagedorn 50 years earlier.29 He presented his operation at the Seventeenth Annual Meeting of the American Society of Plastic and Reconstructive Surgery in West Virginia in November 1948, and he impressed those in the audience, including Barrett Brown and McDowell, with his results.5 Many surgeons subsequently began using his technique, and some developed their own modifications of it, including Wallace Steffensen, who proposed a triangular wedge excision of the medial lip to facilitate inset of the quadrilateral flap. D. Ralph Millard added an ingenious system of measurements for the technique, and Tom Cronin of Houston advocated using the vertical length of the normal side to calculate the length of the cleft side. One criticism of this technique was that it produced an unnatural scar, and another, as stated by Clayton De Haan, was that “measurements made from the cleft side are arbitrary. Even a slight miscalculation in the size of the quadrilateral flap can make the lip too long or too short on the cleft side.”6,32 In 1952 Charles Tennison of Houston introduced two concepts: using a stencil to design a triangular flap and using the Z-plasty principal to gain vertical length. Tennison used a bent paper clip, sterilized for the operation, to figure out the position of an almost-equilateral triangular flap on the lateral lip above the vermilion33 (Fig. 39-12). He described his technique at the Annual Meeting of the American Society for Plastic and Reconstructive Surgery in Colorado Springs and impressed Kirwin Marcks of Allentown, Pennsylvania. Marcks not only adopted this technique but also promoted and popularized it, claiming it was “so much more practical.” He emphasized that this triangle should be placed in the most inferior position where he felt the lip was most deficient.34 The same year that Tennison published his results, A. Duarte Cardoso of São Paulo, Brazil, published a technique which similarly sought to preserve the Cupid’s bow. He noted that the Cupid’s bow on the cleft side was really not missing but was simply displaced upward and needed to be brought down to the horizontal position.35 It is not clear whether Tennison was aware of Cardoso’s contribution, but their ideas complemented one another. Fig. 39-12 The Tennison triangular flap operation created an almost-equilateral triangular flap on the lateral lip, which was drawn with a stencil for precision. Fig. 39-13 Peter Randall’s modifications of Tennison’s triangular flap design included a detailed system of measurements that could be applied to clefts of varying severity. Peter Randall of Philadelphia also adopted Marcks’ technique but made some significant alterations. He observed that in incomplete clefts, there was often only a small amount of displacement of the Cupid’s bow, and he felt that a large triangular flap, as in Tennison’s original description, was unnecessary. Working backward from postoperative photographs, he refined the measurements and developed a mathematical system for designing the lip operation. He reduced the size of the triangular flap and significantly simplified the operation36–38 (Fig. 39-13). This triangular flap approach became known as the Tennison-Randall repair. The triangular flap operation sustained a long period of popularity with many variations. In 1966, Thomas Cronin from Houston described elevation of the lateral triangular flap 1 mm above the mucocutaneous border to facilitate vermilion alignment. David Davies, Jr., of Cape Town, South Africa, advocated two equal flaps of a pure Z-plasty to achieve a predetermined height on the cleft side. Another variation popular in Europe was designed by Tord Skoog of Sweden. He used one triangular flap from the lateral side of the cleft just above the skin vermilion border and a second triangle in the top of the lip just beneath the columella (Fig. 39-14). Later, he put this upper flap inside the nostril into the base of the columella, where the scars were hidden.5,6,38,39 Fig. 39-14 Skoog’s design for unilateral cleft lip repair, described in 1958, put one triangular flap in the lower third of the lip and another just below the columella. The next innovation in unilateral cleft lip repair was the rotation-advancement technique described by Millard.6 The conception of this novel technique is an interesting story. In 1953, Millard was deployed to Korea as a surgeon with the First Division of the Fleet Marines of the U.S. Navy. A Korean man who was working for the Americans learned of Millard’s interest in cleft surgery and brought him to see his 7-year-old son, who had a wide unrepaired unilateral cleft lip. Dr. Millard performed an excellent Le Mesurier repair, but afterward pondered its many shortcomings. The division photographer printed out a number of preoperative photographs of this patient, and Millard worked for hours with these photographs seeking a better solution. One night while working with the prints, he noted: “I had fallen asleep … I opened my eyes … the photographs were standing askew. The angle of its position suddenly made me aware that what we had been searching for had been there all the time!”6 Thus was born the concept of the rotation-advancement technique: the medial part of the cleft simply had to be detached from its high attachments beneath the nose and rotated down to the proper position, and the lateral lip advanced into the gap created by the rotation. Although the parents of other Korean children with clefts were reluctant to bring their children in for surgery, Millard eventually found his first patient for the technique. He playfully “roped” a 10-year-old boy who did not seem reluctant to “play the game.” He was brought to the Quonset Hut Hospital, and without parental knowledge or consent, the first rotation-advancement cleft lip repair was performed.6 Millard presented the rotation-advancement technique at the First International Congress of Plastic Surgery, held in Stockholm, Sweden, in August 1955. Over the ensuing years, he further refined this technique. In his original description, there were three flaps, labeled A, B, and C: A was the medial rotation flap; B, the lateral advancement flap carrying the flared alar base; and C, the small triangular flap attached to the columella which was originally advanced across the nasal floor (Fig. 39-15). One early concern of many surgeons was the persistent shortness of the lip on the cleft side, which resulted in an unbalanced Cupid’s bow. Millard believed that this typically was caused by inadequate rotation of the medial flap, but it led him to introduce the addition of a back-cut at the top of the rotation incision to enable greater downward movement of the medial lip segment. The function of the C-flap then evolved to fill the defect created by the back-cut, and thus to lengthen the columella.6 Fig. 39-15 The original rotation-advancement design conceived by D. Ralph Millard in Korea and presented at the First International Congress of Plastic Surgery in Stockholm in 1955. The rotation-advancement technique overcame many of the disadvantages of earlier unilateral cleft lip repairs: it preserved the Cupid’s bow and the philtral dimple, it improved the nasal tip asymmetry, and the scars were aesthetically camouflaged along the philtral columns and within the alar crease. Since his original description, there have been several refinements of Millard’s original technique, but the basic principles have remained the same. Several surgeons have advocated the addition of a small triangular or rectangular flap from the lateral element into the lower part of the repair to provide additional length, break up the line of the incision, and preserve the contour of the vermilion.40,41 Noordhoff and colleagues42,43 suggested a tiny Z-plasty just above the skin-vermilion junction to re-create the slight transverse depression normally seen just above the white roll. He and others also advocated the incorporation of a triangular lateral vermilion flap to augment the deficient vermilion of the medial lip segment. Some surgeons have objected that the scar produced by the Millard repair obliquely and unnaturally crosses the philtrum in the upper third of the lip. Lester Mohler of Columbus, Ohio, studied the natural philtral shape in children without clefts, and he modified the rotation-advancement technique to reposition this scar, creating a “mirror image” of the philtral column on the noncleft side. In 1987 he reported a study of philtral shape in 100 school children without clefts. He classified them into three groups based on whether the philtral columns were divergent or convergent and, in the latter case, whether they converged at or below columellar-lip junction (Fig. 39-16). Whereas Millard’s rotation-advancement technique produced a shield-shaped philtrum with the scar and unaffected philtral column converging at the midline under the columella, most of the children in Mohler’s study (74%) actually had columns that did not come together in the upper lip. He subsequently altered the design of his repair for such patients in the superior portion of the lip so as to mirror the philtral shape on the noncleft side. In his technique, the rotation incision is drawn in a curvilinear fashion to mimic the shape of the normal philtral column and extended into the base of the columella. A 90-degree back-cut is made in the columella without crossing the normal philtral column, allowing downward rotation of the medial lip segment. The C-flap is advanced into the defect at the columellar base and used to lengthen the shortened columella on the cleft side44 (Fig. 39-17). Several variations of the Mohler repair have been reported, including those by Don LaRossa45 at the Children’s Hospital of Philadelphia, who wrote about a similar approach using curves in unilateral cleft lip repair, and Court Cutting from New York University, who published extensively about his “extended Mohler repair” technique.46 Fig. 39-16 Lester Mohler’s study of different philtral types in normal school children without clefts, showing three primary patterns. Fig. 39-17 Mohler’s operation for varying the reconstructed philtral column depending on the configuration of the column on the noncleft side. Fig. 39-18 Fisher’s design for unilateral cleft lip repair, which places the final scar within the cleft philtral column and superolaterally bordering the lip-columellar crease. A more recent addition to cleft lip repair techniques is the anatomic subunit approximation technique, described by David Fisher47 from the Hospital for Sick Children in Toronto, who published this technique in 2005. Using both the principle of Rose-Thompson lengthening as well as a lower Randall-Tennison type of triangular flap, Fisher designed this repair to maintain the scars at the seams of the anatomic subunits of the lip and nose (Fig. 39-18). Modifications and long-term results of this technique, which are described in detail in a later chapter, have recently been reported by others.48 James Barrett Brown noted that “the bilateral cleft is more than twice the problem of the unilateral, and the results are less than half as good.”49 Accordingly, bilateral cleft lip repair has progressed slowly. The incisions used have evolved from a straight-line closure on each side to various types of flaps like those used in unilateral clefts. Historically, many surgeons would simply replicate their unilateral repair patterns on each side. Some brought flaps back from the lateral side of the cleft to the midline below the prolabium to lengthen the central lip. In 1891 William Rose pared the central tubercle in a V-shaped manner and curved his incisions in the lateral segments, bringing them together in the midline below the apex of the central segment. Le Mesurier applied his quadrilateral flap design to the bilateral defect, also transposing flaps below the prolabium. Brown, McDowell, and Byars introduced a pair of triangular flaps that were brought together under the prolabium and described several variations to accommodate either a long or short prolabium. Louis Schultz of Chicago contributed significantly to the bilateral repair in the 1940s by emphasizing the importance of muscle approximation from the lateral elements behind the central prolabial segment.5 As early as 1790, Pierre Joseph Desault of Paris advocated surgical closure of both sides at the same time after initial premaxillary compression by a cloth bandage. He pared the cleft edges, approximated the lip segments using the prolabium for the central portion of the lip, and fixed the repair with through-and-through sutures in a figure-eight fashion. Both Brown and McDowell followed Desault’s format; they set the premaxilla back and closed both clefts simultaneously. Other surgeons were in favor of a staged repair of the bilateral cleft deformity. Victor Veau felt that, for complicated bilateral clefts, “closure of the entire defect at one time is too formidable,” and he recommended closure of lip and palate in three or more stages, with the lip repaired one side at a time, 4 weeks apart. Others who favored staged repair included Kilner and Holdsworth of Britain and Cronin and Bauer of the United States. These surgeons choose to close the wider cleft first to pull the deviated premaxilla back to the midline.5 The protruding premaxilla was one of the first challenges in the history of the bilateral lip repair. In early repairs, it often was excised completely, leading to a loss of incisors, collapse of the lateral maxillary segments, severe restriction of anterior maxillary growth, and a marked anterior cross bite (Fig. 39-19). As early as 1556, Pierre Franco50 suggested removing the premaxilla completely “with cutting forceps or a small saw, leaving the flesh over them.” This suggestion was echoed by Hendrik van Roonhuyse22 of Amsterdam in 1661, George de al Faye51 of Paris in 1733, and Guillaume Dupuytren52 of Paris in 1833. Pancoast53 did not excise the premaxilla, but instead forcefully fractured it to a better position. In 1844 Malgaigne54 was one of the first to object “to the removal of two, three, or even four incisors.” Other historic attempts to reposition the protruding premaxilla have included removal of the buccal plate of the alveolus, usually with destruction of the incisor teeth. In 1863 Adolf van Bardeleben55 of Germany sectioned the vomer subperiosteally through a small incision, allowing “the sectional septal ends to glide past each other without buckling as the premaxilla was repositioned.” Section of the septum anterior to the vomerine suture, resection of a segment of bone immediately behind the lingual buccal plate, stapling of the prevomerine suture, and a variety of head cups with straps to place static or elastic pressure on the premaxillary segment have all been tried. More recently, orthodontic appliances have been used to reposition the premaxilla. This has been done both actively with screw attachments for retropositioning the premaxilla and for repositioning the lateral maxillary segments and passively with staged dental plates. This approach has now reached a high degree of sophistication and has evolved to include additional appliances to reshape the nasal tip cartilages and to lengthen the columella.56,57 The lip adhesion procedure was another method developed to reposition the protruding premaxilla. First described by Gustav Simon in 1864, this procedure attached flaps from the lateral lip segments to the prolabium to reshape the lip and underlying alveolus before definitive lip repair. In addition to repositioning the premaxilla, the adhesions also acted as tissue expanders of the prolabium, creating more tissue in the central lip segment.6 Peter Randall was a strong proponent of preliminary lip adhesion and believed it achieved the same results as external elastic pressure or internal dental appliances.27,58 Fig. 39-19 A 9-year-old girl who had the premaxilla removed in infancy, with severe maxillary collapse and loss of alveolar tissue presumably caused by a compression apparatus.
A History of Cleft Lip and Cleft Palate Surgery
Peter Randall, Oksana A. Jackson
KEY POINTS
THE UNILATERAL CLEFT LIP REPAIR
Early European History
The Nineteenth Century

The Twentieth Century

The Quadrilateral Flap
The Randall-Tennison Repair
The Rotation-Advancement Technique
The Mohler Repair
Anatomic Subunit Approximation Technique
BILATERAL CLEFT LIP REPAIR
The Premaxilla

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


