Unilateral Cleft Lip and Nose Repair
Kenneth E. Salyer, David K. Chong, Alexandre Marchac, Joseph Michienzi
KEY POINTS
○ Technically skilled surgery must be combined with attention to detail and planning that is conducted in skilled centers with sufficient caseload in an interdisciplinary setting.
○ Cleft lip and nasal deformity are characterized by muscle imbalance, tissue hypoplasia, and asymmetrical skeletal base.
○ Primary lip and nasal correction requires sufficient release of all abnormally attached tissues to allow a tension-free closure and create normal anatomy in three dimensions.
○ The single most important basis of the repair lies in the release of the abnormally attached orbicularis oris muscle, followed by meticulous realignment to allow a balanced lip and a symmetrically oriented alar base and alar cartilage tip projection of the nasal tip.
○ Cleft protocols with long-term outcomes should be reported for speech and growth to help evolve the understanding of maxillary growth and palatal function with respect to surgery.
It is a surgeon’s responsibility, through experience and technical skill, to provide the best possible outcome for each child. This can only be achieved by working with a critical number of cases per year in conjunction with interdisciplinary care over time until the children are completely grown.
The standard for global cleft care should be excellence. Dedicated craniofacial and cleft centers need to be created in strategic locations in developing countries globally. Each center should vigilantly collect data on outcomes of surgical complications, as well as speech and growth. Those who perform isolated care or the occasional operation need to reexamine motives and the ability to transfer care to larger centers in the interest of patient outcomes. The goal for all patients with a cleft is good to excellent facial aesthetics, normal dental occlusion, and normal speech. Long-term outcomes in the literature are sparse. Timing, sequencing, and treatment modalities, including specific surgical techniques, should be validated by measured outcomes, because a surgeon’s best cases are not a reflection of the success of his or her protocol.
The Dallas protocol has been used for more than 40 years and is one proven way that works for our team and patients. This chapter specifically looks at the approach to unilateral cleft lip and palate. A large number of patients throughout the United States have been treated with this protocol at our center. However, although this has generally worked well for patients in the United States, it may not work in other unique locations; optimal protocols that are sensitive to regional needs, travel, availability, and many other factors must be developed individually.
The field of cleft surgery has seen major advances over the last 40 years. Normal function and appearance are now a realistic goal and can consistently be achieved.1 To obtain excellent results, a dedicated team approach, following a surgical, orthodontic, and speech-oriented protocol and built on long-term experience treating patients from infancy through adulthood, is essential. This chapter presents an approach based on more than three decades of experience for the care of patients with primary cleft lip and nose and cleft palate, emphasizing the importance of interdisciplinary treatment over time.
The most important surgical stage when treating a patient with a cleft is the primary cleft lip and nose and primary palate repair; however, much more treatment is needed to achieve consistent excellence. Ongoing treatment by an interdisciplinary team over time, and during the period of growth, is necessary to maintain standards of care. In addition, treatment after the completion of growth is necessary in most cases. Patients with unilateral complete cleft lip and palate are at risk for abnormal growth resulting from cleft dysmorphogenesis and from the healing process from surgical correction.
The cleft lip and nose is an integral part of the problem that must be addressed to obtain a complete repair and excellent result. Several key elements must be considered to obtain the desired result.
First, the nasal involvement is almost ubiquitous and therefore must be addressed primarily at the time of lip surgery.1,2 Second, the treatment should always be interdisciplinary, at a minimum involving a cleft surgeon, an orthodontist, and a speech pathologist when the palate is involved. Third, the problem should be viewed as a dynamic one, extending over the child’s development. Therefore treatment protocols spanning the entire period of growth and development, rather than a one-time “home run” solution, must be the rule rather than the exception.
Our long-term protocol has evolved gradually and has consistently produced good to excellent results. Other protocols result in good outcomes; these results must be shared to allow the evolution of our understanding of growth and speech. A key tenet in removing cleft stigmata is achieving a full, convex, projecting facial skeleton, with minimal soft tissue scarring and normal vocal resonance and articulation. Each cleft surgeon has one or two opportunities to change his or her protocol based on an honest review of results, which mandates vigilant recordkeeping. Treatment protocols develop over time, and they should be based on ongoing experience, continuous critique, and an accepting attitude to improvements. In a 40-year career, this translates to two generations of patients followed through growth completion and really allows only two or perhaps three protocol changes to be fully evaluated. Thus the experience gained must be passed on to the next committed generation of surgeons.
Early nasal reconstruction plays an essential role in enhancing patients’ self-esteem from an early age, and this has become my (KS) standard of care in the treatment of patients with unilateral cleft lip and nose and cleft palate. Despite the reluctance of some surgeons to perform early nasal surgery, simultaneous lip and nose reconstruction eliminates the need to correct severe secondary nasal deformities that develop with maturation and growth, producing a thickened skin with more distorted structures and less pliable, cartilaginous framework.3 Early lip and nose repair, followed by early palate closure, provides the foundation for long-term excellent results.
Whatever protocol and surgical technique is adopted, the surgeon’s experience, talent, and attention to detail are important factors in determining the final outcome of cleft lip and nose repair.4 Achieving a smooth, seamless contour between two edges or 0.1 mm of inadequate rotation can consume an obsessive cleft surgeon in the quest for perfection. Releasing and repositioning all the displaced nasal and lip elements in all three planes in space plagues the surgical eye and requires that the surgeon observe the repair from multiple angles. One of the most common causes of secondary deformity is inadequate release of all the displaced components of the lip and nose, resulting in incomplete reconstruction and alignment.
Over the past three decades, as a result of refined techniques, careful surgery, and the avoidance of scars, primary nasal correction at the time of lip repair has received increasing attention.4–6 In 1970 I developed a primary cleft lip nasal repair incorporating cartilage repositioning, and this has been improved upon since then. Numerous studies have also disproved the myth that early nose tip surgery negatively affects cartilage growth.1,4–10 It has also been shown that early nasal surgery sets the stage for more symmetrical growth of the nasal cartilages, and if a final rhinoplasty is required after nasal growth is complete, the deformity at that time is less severe and will more likely have a better final result.
ANATOMY
Functional reconstruction of a cleft lip should be based on a good knowledge of the muscular deformity of the lip. The current trend of muscle mobilization and accurate surgical repair of the orbicularis oris muscle in unilateral cleft lip is based on an understanding of the muscular anatomy in this deformity. Several authors, including Randall et al,11 Kernahan,12 and Nicolau,13 emphasized the importance of the orbicularis oris muscle in lip reconstruction and described their methods of repair. Park and Ha14 thought that the inaccurate and mixed connection between the two different functional muscular components makes the repaired lip distorted and unbalanced. They believed this could get worse during growth and stressed the importance of accurate repair of the superficial and deep portions of the muscle. We think that release of the abnormally attached muscles is necessary, with realignment and proper approximation, with compensation for deficiencies. Identification of the specific portions of the cleft muscle is not necessary; however, a full release and reconstruction of the muscle, as a component of the lip and vermilion, is crucial to success for proper alignment of the lip and nose. This is the single most important step in achieving a balanced lip and nose repair. Positioning the muscle properly provides balance and three-dimensional symmetry of the face, both when static and with dynamic motion.
Normal Upper Lip
The presence of two well-defined and functional components of the orbicularis oris muscle is well described.12–15 They consist of the superficial (pars superficialis) and the deep (pars marginalis) components. The superficial part (pars superficialis) is located under the skin of the lip and is related to other facial muscles of expression (levator labii superioris, alaeque nasi, and zygomaticus minor), and these retract the upper lip as a group. The superficial portion of the muscle consists of an upper and lower bundle. The upper bundle represents the common insertion of the muscles of facial expression and itself inserts onto the anterior nasal spine, septopremaxillary ligament,16 and the nostril sill, passing deep to the alar base. The lower bundle derives its fibers from the depressor anguli oris muscle on each side and decussates in the midline, inserting in the skin and forming the philtral ridges of the contralateral side.
The two portions of the orbicularis oris muscle thus correspond to the double function of the upper lip. The deep part (pars marginalis), extending from one modiolus to the other, seals the mouth as a constrictor, whereas the superficial part (pars superficialis) mingles with the extrinsic facial muscles to open the mouth as a retractor.
Contraction of the pars marginalis when the mouth is pursed, thickens the vermilion and lengthens the upper lip height. Simultaneous relaxation of the pars superficialis produces perioral fine wrinkles and accentuates the philtral columns, while flattening the nasolabial folds. In contrast, when the mouth is opened, the contraction of the pars superficialis leads to flattening of the perioral wrinkles and philtral columns and accentuates the nasolabial fold. In addition, the upper lip height shortens. Simultaneous relaxation of the pars marginalis decreases the thickness of the vermilion.14
Unilateral Cleft Lip
Nicolau13 and De Mey et al,15 in electrical stimulation and histologic studies, respectively, showed that the superficial part of the muscle, which normally inserts on either side of the midline, is misdirected by the cleft. On the cleft side, the lower bundle of the pars superficialis passes from the commissure toward the midline but changes direction at the level below the displaced alar base to run almost vertically and be abnormally attached to the nostril and the periosteum of the piriform aperture. Contraction of the muscle results in a significant lateral bulge. The upper bundle of the pars superficialis is attached to the lateral aspect of the nasal ala and the nasolabial fold, thereby contributing to the nostril deformities, whereas the pars superficialis on the noncleft side appears not to be affected by the cleft. The muscle fibers are scarce and run transversely. A portion of the fibers inserts almost perpendicular to the cleft edge; others insert into the deep dermis. Contraction of this part of the muscle re-creates philtral ridges and retracts the free margin of the cleft. Although this part of the muscle appears to be normal and not affected by the cleft, its unopposed lateral and upward pull likely contributes to the anterior septal deformity.
Both studies showed that in both incomplete and complete clefts, the pars marginalis, which is located in the vermilion, is minimally displaced. It is simply interrupted by the cleft and ends in the submucosa.
PATHOGENESIS OF CLEFT LIP AND NASAL DEFORMITY
Three major factors influence the nasal deformity in both complete and incomplete unilateral clefts: (1) muscle imbalance, (2) tissue hypoplasia, and (3) asymmetry of the skeletal base.17
Muscle imbalance affects nasal symmetry in both complete and incomplete unilateral cleft lip and nose, by distorting the position of the alar base and the shape of the nostril. With a partial or complete discontinuation of the orbicularis oris muscle in unilateral cleft lip and nose, the extrinsic muscles of facial expression, which are attached to the orbicularis oris muscle on the cleft side, pull the alar base more laterally compared with the noncleft side. The existing muscle imbalance also changes the position of the alar cartilage, as well as the orientation of the nostril, from an oblique to a horizontal orientation. Because of the insertion of muscle on the base of the septum and columella on the noncleft side, contraction of the muscle pulls the septum and columella toward the noncleft side. Thus the severity of the cleft nasal deformity depends on the degree of separation of the orbicularis oris. Proper repair of the muscle during primary lip repair does not necessarily improve the existing nasal deformity. As the lower lateral cartilage is displaced, lip muscle repair must be combined simultaneously with repositioning of the alar base and lower lateral cartilage.
Skeletal hypoplasia occurs in complete clefts and occasionally in partial clefts, despite the alveolus and palate seeming to be unaffected. Hypoplasia of the lesser maxillary segment occurs most commonly along its edges, as well as along the ridge of the piriform aperture. This further accentuates the nasal deformity with the skeletal imbalance and asymmetrical alar base.18
Malposition of the maxillary segments leads to a nasal deformity that involves all structures of the nose on the cleft side, including the septum. Often the hypoplastic lesser maxillary segment not only leads to malpositioning of the alar base posteriorly and inferiorly, but it can also stretch the alar base horizontally, resulting in flattening and elongation of the nostril with typical downward deflection of the lateral crus of the alar cartilage. The orientation of the medial to lateral crura of the alar cartilage on the cleft side is also changed. Because of the force of lateral and inferior pull, the medial crus is shorter and the lateral crus longer on the cleft side than the noncleft side, since the break points defining the length of each segment are changed. The alar cartilage is buckled and deformed. It is rotated downward and drawn into an S-shaped fold. The distortion of the alar cartilage, depending on its severity, can be very difficult to correct during primary lip and nose repair. Salyer et al,7 Anderl et al,4 and McComb6 have successfully corrected this deformity using their individual techniques. As a result of the lateral and inferior pull, as well as from the deformed alar cartilage, the dome on the cleft side is more obtuse and lower than on the noncleft side. The columella is shorter because of the shorter medial crus of the alar cartilage on the cleft side. The columella is also pulled to the noncleft side by the orbicularis oris fibers entering its base.
Septal deformity is common, and its severity varies. The caudal septum is usually deviated to the noncleft side, as the base of the septum is dislocated from the groove on the maxillary crest; the deviation may lead to posterior nasal obstruction on the cleft side. The degree of obstruction can be presumed by the distortion of the nose.
The following characteristics are typical of a unilateral cleft lip and nose deformity. The degree and severity of the deformities vary, and all are not present in every patient (Figs. 43-1 through 43-3).
- The columella is shorter on the cleft side, with its footplate displaced and tethered inferiorly.
- The base of the columella is deviated to the noncleft side.
- The medial crus of the alar cartilage is shorter on the cleft side.
- The lateral crus of the alar cartilage on the cleft side is longer and, together with the adherent skin, drawn to an S-shaped fold.
- The alar cartilage on the cleft side is displaced in the backward and downward planes.
- The nasal tip is displaced and asymmetrical, with loss of the defining point on the cleft side.
- The dome on the cleft side is obtuse.
- The flattened ala results in horizontal orientation of the nostril on the cleft side, and it is usually larger than the opposite side.
- The entire nostril is retropositioned.
- The base of the ala is displaced posteriorly and inferiorly, where it is tethered to the displaced underlying bone on the cleft side.
- The nasal floor is lower or absent on the cleft side.
- The caudal septum and anterior nasal spine are deflected to the noncleft vestibule.
- Septal deviation of varying degrees leads to posterior nasal obstruction on the cleft side because of the deviation of the septum and, often, the narrowing of the internal nasal valve.
- The lower turbinate on the cleft side is hypertrophic.
- A nasolabial fistula may be present.
- The lesser maxillary segment is hypoplastic and displaced on the cleft side.
- The nasal pyramid is asymmetrical.
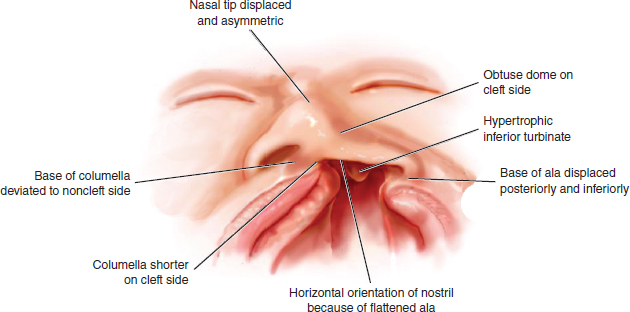
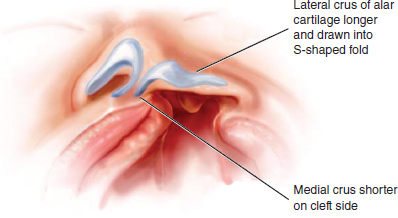
Fig. 43-2 Anatomy of the cleft side alar cartilage.
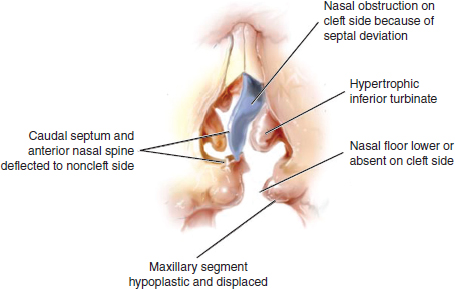
Fig. 43-3 Anatomy of the cleft septum, turbinate, and skeleton.
KEY CONCEPTS IN CLEFT LIP AND NOSE REPAIR
Lip Adhesion
Preliminary lip adhesion in the unilateral complete cleft lip, advocated as early as 1954 by Johanson and Ohlsson,19 was mainly popularized by Randall20 in the late 1960s. Preliminary lip adhesion decreases the tension of definitive lip closure through its molding effects on the maxillary segments. Seibert21 discussed the principles of lip adhesion and the possible benefits of the procedure. He recommended minimal soft tissue undermining of the lateral maxillary segment.
Randall20 suggested that short broad triangular flaps be interdigitated and sutured together at the mucosa, muscle, and skin layers. Millard,22 on the other hand, proposed a high adhesion, preventing a scar in the area of the repair and introducing lateral lip parings into the lateral nasal vestibule. Millard2 advocated lip adhesion as a substitute for presurgical orthopedics and incorporated some nasal correction in the adhesion.
It has been our experience that lip adhesion may contribute to unnecessary additional scarring and abnormal tethering of the lip or nasal elements, and we find it unnecessary.7 Early in our experience, we retrospectively evaluated 50 patients in a blind fashion, comparing the aesthetic results of those who received lip adhesion with those who did not. We found improved aesthetic outcomes in the group that did not undergo lip adhesion, so we have abandoned the use of lip adhesion in our treatment protocol. I (K.S.) have not performed a lip adhesion since our study was completed in 1977. Still, many experienced cleft surgeons continue to use preliminary lip adhesion to treat the abnormal skeletal base and facilitate definitive closure of the lip and nose.23,24 We think that although lip adhesion may make it easier for the surgeon to close the lip, it comes at the potential expense of the overall aesthetic result. Lip adhesion may actually cause fixation or scarring of the alar base and associated adjacent structures in an abnormal position, making it more difficult to obtain a definitive normal contour of the nose.7 Others have reported benefits to the use of lip taping as a form of “nonsurgical” lip adhesion.25 The current popular use of presurgical orthopedics and nasoalveolar molding has largely eliminated the need for lip adhesion; therefore lip adhesions may be used less by surgical teams.
Timing of the First-Stage Repair
The initial repair of the lip and nose sets the foundation for the appearance and the growth of the face. Every cleft team advocates slightly different timing, ranging from neonatal repairs to reconstructions at 6 months of age or older.
Intrauterine repair of the cleft lip has been contemplated for 25 years and has been stimulated by the experimental findings in fetal surgery that wounds created in the ectoderm of the fetus, very early in gestation, heal clinically and histologically without scar formation. Although this phenomenon is not clearly understood, it is believed to be related to the absence of cellular inflammatory response by the fetus, no collagen deposition, no wound contraction, and healing by what appears to be regeneration. Hallock26 and Longaker et al27 conducted ovine and mice trials to prove the feasibility of antenatal cleft surgery, with the theoretical benefit of a complete absence of scarring. As Longaker demonstrated histologically with his ovine model, in utero repair of clefts can indeed be scarless. However, antenatally repaired clefts have resulted in lips that were significantly shorter than their contralateral noncleft sides. Antenatal surgery prevents the vitally important identification of landmarks required to enable a balanced lip and nose repair. The theoretical advantage of an invisible scar would be more than counteracted by the lack of balance and proportion that a later procedure enables. This degree of lip shortening would require a secondary lip revision, thereby defeating the purpose of performing an intrauterine repair. Ortiz-Monasterio28 attempted a human antenatal cleft repair but was discouraged from performing further cases because of the life-threatening situation for the fetus and the mother. The attendant risk of fetal loss is such that, at the present time, intrauterine fetal surgery should be reserved for significant or life-threatening malformations that cannot be treated as well by postnatal intervention.
Several teams perform lip repair in neonates, based on Vanwijck’s finding of an optimal healing period for mice with minimal collagen production in the late fetal stage, which lasted 2 days after birth.29
It has been our experience—and a common theme among many cleft centers—that 3 to 6 months of age is a good time to perform the initial cleft lip and nose repair. At this time, the infant has developed beyond 60 weeks’ gestation, which many pediatric anesthesiologists consider a “safety border” of maturity when considering general anesthesia. In addition, the lip has grown, and this facilitates greater precision in the repair. Finally, the parents have had time to psychologically accept their child’s malformation, which has been shown to be a key point in a long-term treatment protocol.30 Our center has performed lip and nose repair in newborns and at 6 weeks, but we believe that at this early age, the tissues have not matured adequately in most infants. In our experience, the results of lip and nose repair before 3 months of age are not as good or accurate as those performed after 3 months of age.
Skin Incision
The skin incision is not very important in and of itself. The final aesthetic and functional outcome is determined by the extended dissection that allows the surgeon to free all the anatomic elements of the lip and nose displaced by the clefting to achieve complete repositioning of these elements. The concept of the Salyer lip and nose repair is one of totally freeing all elements of the lip and nose in a plane above the periosteum, so they are floating free above the abnormal skeletal base. The lip and nose elements are then placed in the proper position in relation to the three-dimensional reconstruction, attempting to make form and function as normal as possible. The aesthetic result always remains foremost. Repositioning the muscle is one of the keys to achieving a good and stable result; this provides the foundation and support of the repair, maintaining the alar base and nasal tip projection and symmetry. Lining up the muscle is the single most important maneuver in the repair; it should be vigilantly aligned. Any underrotation or overrotation of a carefully planned repair is usually the result of a misaligned muscle repair. The muscle alignment is more important than the design of skin incision in achieving an excellent result.
Many skin incisions have been described since Malgaigne,31 who introduced the concept of closure of the cleft lip by local flaps in 1861. Various current techniques emphasize exact preoperative markings that to some extent commit the surgeon to incisions. However, the repair should be fluid, allowing improvisation and artistry by the surgeon, especially with respect to the nose. For 20 years we thought that an incision around the alar base was necessary to reshape the ala; however, we have now entirely eliminated this incision, because it only adds an unnecessary scar.
Supraperiosteal Dissection Versus Subperiosteal Dissection
Two schools of thought exist in cleft surgery regarding extensive dissection and repositioning of the lip and nose elements. In 1978 the French surgeon Delaire,32 dissatisfied with his results, went back to the principles stated by Victor Veau,33 one of the pioneers of cleft surgery. Delaire’s technique involved a careful dissection of all muscles affected, anatomic repositioning of the lip and nasal entrance structures, and a wide subperiosteal dissection.32 The anatomic subperiosteal plane is easy to find, and the dissection is carried up to the infraorbital nerve. This maneuver, combined with periosteal relaxing incisions, allows primary closure of wide clefts.
Mannucci et al34 demonstrated that neither the supraperiosteal nor subperiosteal undermining of the anterolateral surface of the maxilla seems to interfere with maxillary growth in rabbit models, but this has not been proved in humans. Bardach et al35 demonstrated that lip scarring inhibited facial growth in beagles, but these variables have not been fully evaluated in the cleft population.
Without clear evidence about the implications of growth, preperiosteal dissection offers the advantage of allowing the tissue to move more easily, which is especially important in wider clefts. The analogy can be drawn to a scalp flap, which mobilizes with greater freedom when raised in a preperiosteal plane versus a subperiosteal plane.
Nose Repair
As discussed previously, correction of the nasal cleft deformity is a necessary and integral part of the primary surgery. It sets up facial balance, and an asymmetrical nose can carry as great a stigma as a lip that is poorly aligned. Long-term studies have clearly demonstrated the effects of lack of growth disturbance from a carefully dissected primary nasal repair.
The cleft nose deformity, affected by the skeletal base and deformed alveolus, maxillary segments, and palate, includes several components, including the alar base, the medial and lateral crus of the alar cartilage, the nasal dome, the columella, and the nasal septum. The severity of the primary nasal deformity is intimately related to the degree of displacement, abnormality, and hypoplasia of the maxillary segments. Continued hypoplasia and displacement of the maxillary segments (particularly the lesser segment) results in varying degrees of maxillary deficiency with subsequent growth and development. The final outcome depends not only on the cleft dysmorphogenesis, but also on the selection, sequencing, and execution of surgical procedures.
Complete rehabilitation must address three dimensionality, as well as growth over time, to obtain the desired final result. In our experience, hypoplasia of the lesser segment results in an occlusal cant and maxillary deficiency, which necessitates definitive orthognathic and orthodontic correction to achieve facial balance and symmetry. Lesser segment deficiency is a key limiting factor in long-term outcomes in the unilateral cleft lip and nose and cleft palate patient; this inherent hypoplasia may prevent a perfect or excellent result. Shetye36 has recently demonstrated the lack of growth of the lesser segment in patients with clefts. Subsequent studies have shown a 15% volume deficiency of the lesser segment.7
Hypoplasia of the lesser segment, or base, of the cleft nose results in displacement of the lower lateral cartilage laterally and inferiorly on the cleft side. The nasal dome is flattened and slumped in a downward position. The alar cartilage on the cleft side is flat, giving it the false appearance of having greater length when compared with the other alar cartilage, which also is abnormally displaced to the noncleft side. The relationship of the lower lateral cartilage to the septum is normal; however, the septum itself is deformed, thereby tilting the base of the nose toward the noncleft side and the tip of the nose toward the cleft side.
This raises the question of whether the septum should be repositioned or surgically addressed at the time of primary lip and nose repair. Some surgeons, including Anderl et al,4 believe in addressing the septal deformity at the time of primary lip and nose repair; however, it is a technique that should be evaluated in greater detail. We have found passive perisurgical orthodontics improve septal position. If the septum remains deviated at the time of surgery, we relocate the anterior portion of the septum and affix it to the anterior nasal spine (ANS). We are currently conducting long-term analysis of these results.
The key to correction of the cleft nasal deformity is the dissection that frees the alar cartilage and its attached vestibular lining and the repositioning that translocates it into a normal position. These maneuvers establish the normal nostril vault and alar cartilage shape.1,5,6 At this stage, the major deformity of the nose is corrected. By combining this dissection and repositioning of the alar cartilage with complete freeing of the soft tissue envelope of the nose and the correction of the alar base and floor of the nose, consistently good results may be achieved at the time of primary correction. At this time in our protocol, the abnormal skeletal base and deformed septal cartilage (except for the anterior portion) are ignored, while the displaced soft tissue and cartilaginous elements of the lip and nose are anatomically aligned.
Although those who advocate presurgical orthopedics attempt to improve skeletal alignment before lip and nose repair, the long-term outcomes with respect to facial growth must be evaluated. Berkowitz et al37 have demonstrated growth abnormalities in patients treated with the Latham-Millard POPLA (active presurgical orthopedics, gingivoperiosteoplasty, and lip adhesion) procedure. Many patients therefore need definitive orthodontic care and skeletal surgery once growth is complete.
Airway Opening and Nasal Stents
For 20 years, Talmant and Luineau38 did not agree with the widely spread opinion attributing poor results to severe hypoplasia from the cleft itself. Talmant believed these patients possessed normal growth potential but needed normal function to show it and that oral breathing, so common among these patients, was enough to explain their poor growth. He attempted to restore normal nasal physiology through precise secondary surgery of the nostril and the septum as early as 6 years of age with some encouraging results.
However, with experience, Talmant and Lumineau38 concluded that changing the habit of oral breathing is particularly difficult in cleft patients, and that nasal breathing should be established after the primary surgery to prevent compensatory mechanisms and their consequences. Talmant therefore emphasized the importance of opening the airway during primary cleft surgery by shifting the septum into a normal position and maintaining the nostril airway by soft nasal stents placed after the primary closure—thereby combining functional and aesthetic outcome.
We also advocate the use of nasal stents postoperatively.7 They are inserted at the time of primary suture removal 1 week postoperatively. This technique splints the nostril with silicone conformers to limit the effects of scarring and wound contracture and improves the nasal airway. The splints are worn for 3 months to diminish scarring and vestibular stenosis in primary cases while improving nasal breathing. The Koken stent is used for primary and secondary cases.
Tissue expansion can also be used for preoperative nostril expansion in patients with unilateral cleft lip and nose defects, although it is time consuming and labor intensive. Nasoalveolar molding (NAM) is advocated by a number of centers for unilateral cleft lip and nose deformity; however, we have obtained excellent results consistently without adding this technique. Molding of the nose with NAM must be done carefully to prevent creating a meganostril through the potential tissue expansion effect, rather than just the desired reshaping of the nostril.
Facial Growth
In contrast to the poor maxillary growth infants display after primary lip and nose surgery, unoperated adults with cleft lip and palate have historically exhibited good facial growth.36 It has been demonstrated more recently, however, that facial growth in patients with an unoperated cleft is not entirely normal. A strong consensus exists that scarring from primary surgery is the main cause of maxillary hypoplasia, particularly scarring from secondary epithelialization of denuded palatal bone or from closure of the cleft in one layer.39
Many, sometimes controversial, protocols have been developed to improve the outcome of facial growth. Some teams use the Goslon yardstick, in which dental models of patients being treated with the same cleft protocol are taken; the incisal relationships are then compared at various ages. Although the analysis has some merit, once orthodontic intervention is commenced (which in some centers is as early as 5 years of age), the assumption that incisal relationships reflect maxillary growth can no longer be made.
The differences between the various treatment protocols reflect the personal influence of each surgeon and team. At a recent cleft meeting in Oslo, Norway, a group of 10 experienced senior surgeons all agreed that the single most important factor in determining outcomes was not the treatment protocol or the sequencing, but the surgeon’s skill, combined with a multidisciplinary team approach.
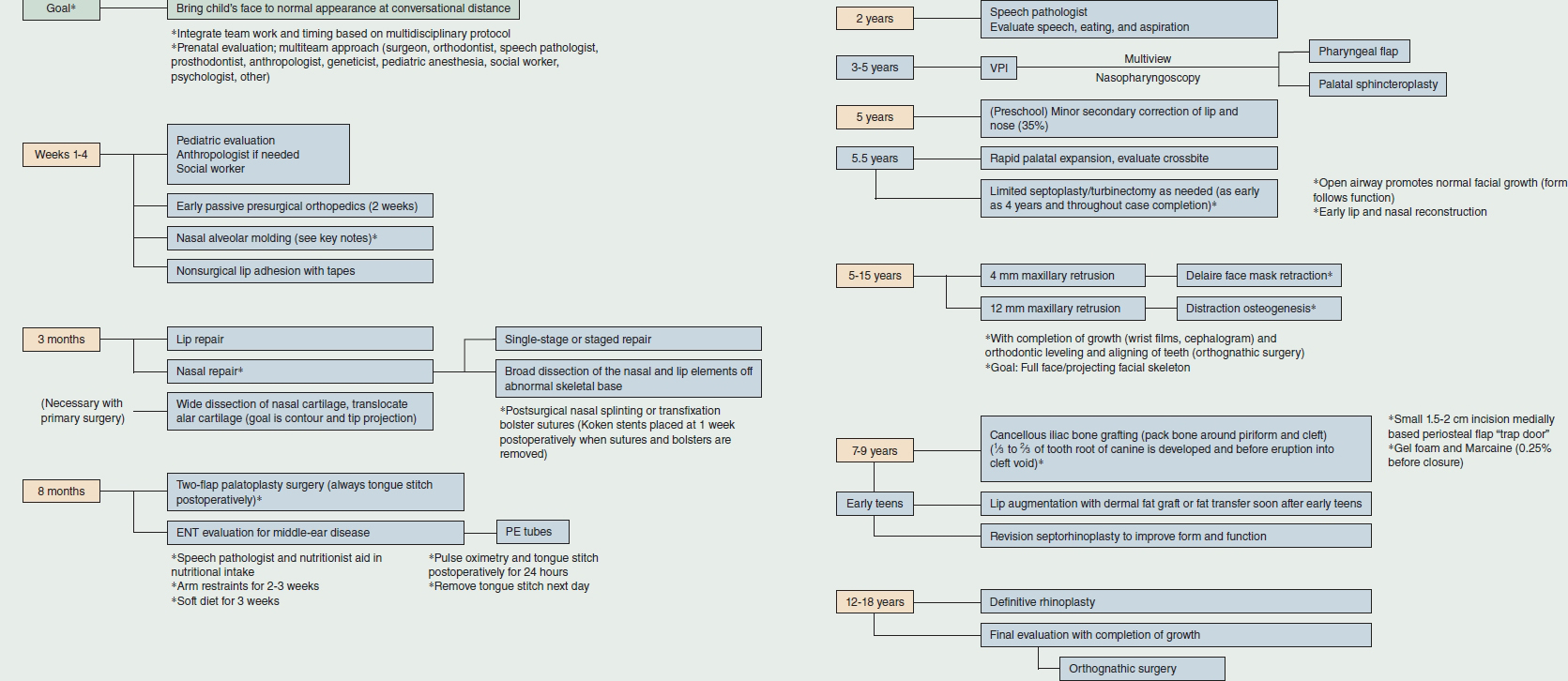
PROTOCOL AT OUR CENTER
Passive presurgical orthopedics is begun at 2 weeks of age at our center. Other than the use of the passive device, the abnormal skeletal base is mainly ignored at this stage, and emphasis is placed on the soft tissue repair of the cleft lip and nose complex.
The primary cleft lip and nose repair is performed at 3 months of age, as previously discussed. When the palate is involved, two-flap palatoplasty is performed at 8 months of age.40 Recent long-term outcome data indicates normal speech is attained in more than 90% of patients treated with this protocol. Approximately 35% of my (KS) patients benefited from minor secondary correction of the lip and/or nose, generally performed at preschool age, or around 5 years old.
In most cases definitive rhinoplasty is performed at or after completion of growth. This provides definitive normal function and appearance.
Palatal expansion is performed at 5.5 years of age, followed by cancellous iliac crest bone grafting when one third to two thirds of the root of a tooth destined to erupt in the defect has developed. Importantly, this is performed before its eruption into the cleft void. Bone grafting at this stage provides adequate bone for the orthodontist to achieve orthodontic restoration in 95% of the cases.
An open airway promotes normal facial growth; therefore, limited septoplasty and turbinectomy are performed as needed, from the early age of four to five until completion of care.
If maxillary sagittal growth is delayed because of the cleft dysmorphogenesis or scarring, we perform one of two procedures between 5 and 15 years of age. For those patients with up to 4 mm of midface retrusion at the occlusal plane, a Delaire face mask is used for protraction. With retrusion of 12 mm or more, we perform distraction osteogenesis.7 To achieve optimal facial balance and aesthetics, orthodontic alignment and leveling of the teeth are performed; furthermore, at skeletal maturity, approximately 40% of the patients in our protocol undergo orthognathic surgery. This number has increased as we strive for entirely normal, stable occlusion in all patients (Fig. 43-4).