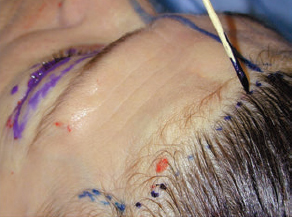
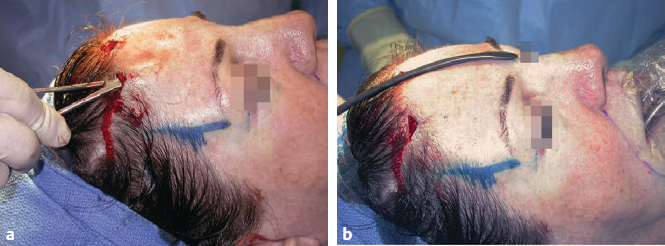
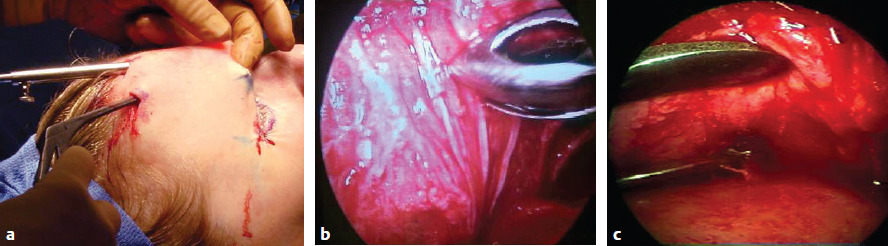
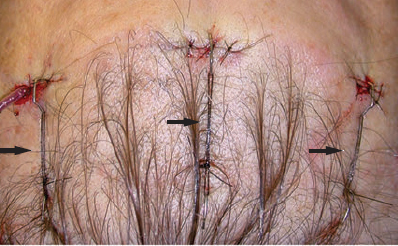
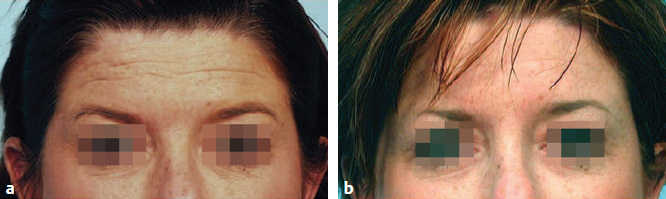
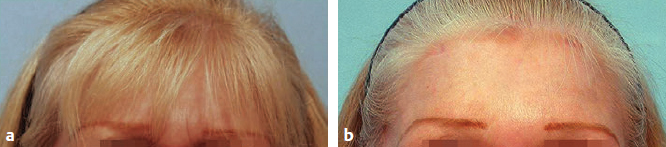
CHAPTER Patients who present for an aesthetic facial improvement, in many instances, are not aware of the factors that lead to an aged or “tired” appearance. Most of the time they focus on the midface and periorbital changes. It is the clinical responsibility of the surgeon to recognize forehead and brow ptosis and demonstrate to the patient how it can be improved. A forehead lift procedure results in several improvements to the aging face. It raises the eyebrows to a more youthful level, ameliorates the transverse and vertical wrinkles, and opens up the eyes. These changes work very well in complementing the facelift. Wrinkles develop because the muscles insert into the skin. Young skin is elastic and wrinkles are fleeting and temporary; as the skin ages, it becomes inelastic, and wrinkles become permanent. The muscles of the face are unique. They do not have a bony origin and bony insertion. They have no fascia. Thus they do not have an all-or-none total contraction. They may contract only portions of the muscle, which allows the multitude of facial expressions. The frontalis muscles are paired muscles located just below the subcutaneous tissue and on top of the galea. Each muscle’s origin and insertion are into the skin, and it extends only to the frontotemporal ridge. Therefore its contraction results in transverse forehead wrinkles. It is the only elevator of the eyebrows. As opposed to the single brow elevator, three muscles depress the brow: the procerus, corrugators, and portions of the orbicularis oculi muscle. These muscles have a bony origin and insertion into the skin. They are responsible for vertical and transverse glabellar creases. Their combined action lowers and converges the medial aspect of eyebrows. According to the cadaveric studies performed by Knize,1 the transverse head of the corrugator produces vertical frown lines and contributes to oblique lines, whereas the oblique head of the corrugator, depressor supercilii, and medial head of the orbital portion of the orbicularis oculi muscle depress the medial eyebrow and contribute to glabellar oblique lines. The eyebrows begin to droop early in life (28 years). With aging, the medial aspect converges and the tail of the eyebrow raises (because of overaction of frontalis muscle). As described by Kaye,2 the eyebrows are a critical part of facial expression. Therefore correction, in general, should be done as a unit. In special circumstances, the technique may be adjusted to improve results—for example, a little extra lifting in the central part of the flap in a perpetually angry-looking patient or in the lateral portions of the flap in a patient that always looks sad. On the other hand, if too much tension is created in parts or in the entire flap, inadvertent changes in expression may occur. For example, excessive brow elevation medially may result in a sad look, excessive elevation centrally or totally may create a surprised or startled look, and excessive elevation laterally could produce an angry look.2 Summary Box Unfavorable Results and Complications of Browlift • Scalp numbness • Dysesthesia • Vertical and transverse glabellar creases • Poor eyebrow elevation • Scalp necrosis • Alopecia • Hematoma • Front nerve injury • Inadequate amelioration of wrinkles • Infection • Inability to close eye • Overelevation of eyebrows An open technique consists of excision of an ellipse of skin and subcutaneous tissue, varying from partial to complete excision of the forehead muscles. The type of incision and size of the resection is planned according to the desired elevation and patient characteristics. For bald patients or those with more than 5 cm between the brow and hairline,3 the incision is placed the level of the hairline, which will result in shortening of the forehead. According to Connell and Marten,4 every 1 mm of eyebrow elevation produces 1.5 mm of elevation of the hairline (Fig. 20.1). In patients with a low hairline, a coronal incision in the hair-bearing scalp is chosen, with the incision placed perpendicular to the hair follicles to allow the growth of hair through the scar.5 Once the incision is made, a subperiosteal dissection will provide the most solid elevation, whereas a subcutaneous approach will remove the skin attachments to the muscle, directly addressing the transverse wrinkles (Fig. 20.2). Several approaches have been described with particular advantages and disadvantages. These include superciliary, midforehead, coronal, transblepharoplasty and temporal. The superciliary approach consists of direct excision immediately above the brow with the intent of hiding the scar at the superior margin of the brow, avoiding the visibility of the other forehead scars in bald patients. Another principle behind this technique is the elastic band principle suggested by Flowers et al,6 which asserts the farther away the suspension point, the less effective the lift. Fig. 20.1 Markings before the hairline incision. Fig. 20.2 Excess skin after plication. (a) Before plication. (b) After plication. A midforehead lift consists of direct excision of a transverse strip of skin in the forehead. The rationale for this incision is based on patients who have deep forehead rhytides that can hide the scar and patients with male pattern baldness, in whom a coronal lift would be troublesome. It is particularly beneficial in bald patients and should be avoided in patients with a short forehead, because it advances the hairline forward. A coronal incision must be hidden in the hair-bearing scalp and planned further posterior in balding males. It is best suited for patients with a short forehead and low hairline, because elevation of the brow will result in elevation of the anterior hairline to a higher magnitude (Fig. 20.3). Fig. 20.3 Results of a previous coronal and temporal browlift that caused hairline elevation, scarring, and alopecia with scalp paresthesia. Temporal browlifting was initially described as an extensive subcutaneous undermining in the temporal and lateral orbital areas up to the anterior branch of the temporal artery, at which point the dissection deepened to a subgaleal plane, with the most common complication being alopecia.7,8 Modifications of this technique included using the subgaleal plane and extension to the zygomatic arch for an added midface lift9,10 (see Fig. 20.3). The goal of a transblepharoplasty incision is to generate an inconspicuous scar; to elevate the brow by transecting its attachments to the orbital rim, suspending it superiorly; and to partially or completely resect the procerus, corrugator, and depressor supercilii muscles through a blepharoplasty scar.11–16 The long coronal incision of an open technique divides branches of supraorbital nerves, resulting in permanent scalp numbness and occasional dysesthesia, in addition to leaving a long incision. Because it elevates the forehead and sideburns, it is a poor choice in patients with a tall forehead, for whom an endoscopic approach will result in more appealing results. Another disadvantage is the partial excision of the frontalis muscle to ameliorate the transverse wrinkles, because it is the only elevator of the eyebrows. Because of the poor visualization, the open technique often results in minimal division or excision of corrugators and procerus muscles, which leads to persistence of vertical and transverse glabellar creases. The poor visualization also does not allow a complete division of the periosteum, which is essential to elevate the eyebrows. Scalp necrosis is rare. However, alopecia is fairly common and of varying severity. With the advent of endoscopy, a minimally invasive approach to address mild to moderate brow ptosis was developed (Video 20.1). It is especially suited for patients with elastic skin who do not require skin excision. This method is based on ablation of the depressors of the eyebrow, enhancing the unopposed effect of the frontalis muscle and division of the supraorbital periosteum to reposition the eyebrows freely.17,18 Additional eyelid procedures (e.g., blepharoplasty, eyelid ptosis) are completed before the endoscopic intervention so the eyelid surgery is not compromised by edema from previous interventions. Three minimal-access incisions are placed at the frontal prehairline level, one at the midline and the others at the level of the lateral limbus. Triangular incisions with transverse closure achieve some elevation of the eyebrows and permit easier entrance of the endoscope. The size and shape of the triangular excision matches the estimated brow elevation desired (Fig. 20.4). Subperiosteal dissection extends to the supraorbital rims and to the frontotemporal line. Dissection is extended further to the nasal tip to release the procerus. The periosteum is divided at the supraorbital level with a blunt periosteal elevator and a hook knife (carpal tunnel knife). (Fig. 20.5). Ablation of the corrugators and procerus and more limited excision of other depressors is achieved with a grasp forceps. The supratrochlear and supraorbital nerves are identified and preserved (Fig. 20.6). After transverse closure of the access ports, temporary suspension is achieved with cable sutures secured from the skin incisions to the scalp for 3 to 5 days. This period allows for adhesion of the periosteum and a long-term effect. The resection of the depressor muscles obviates the need for other methods of suspension (Fig. 20.7). Fig. 20.4 The typical triangular incisions, used as endoscope sites and located anterior to the hairline. Fig. 20.5 (a) Subperiosteal plane entered through the frontalis with a hemostat. (b) Dissection extending to the lateral orbital rims with a blunt dissector. Fig. 20.6 Muscle ablation. (a) An external view of the forceps clamp in place with digital counterpressure. (b) The endoscopic view of the brow depressor muscles in the glabella and between the supratrochlear and supraorbital nerves. (c) The final result, with muscle excision, periosteum division, and intact nerves. Fig. 20.7 The transverse closure of the triangular skin incisions with temporary suspension with sutures and staples, resulting in a “functional” suspension. We consider this to be a more physiologic operation, a true balancing operation, which requires knowledge of the location and function of the forehead musculature. This approach provides better visualization of the supraorbital and supratrochlear nerves with endoscopic magnification and high definition endoscopes. Scalp numbness is temporary, with minimal dysesthesia. Frontal nerve injury is exceedingly rare, with only 2% demonstrating temporary paralysis.19 Because no skin excision is made, the vertical height of forehead is not increased. The technique prevents hyperelevation of the eyebrows, except in cases when more permanent fixation is used (e.g., miniplates, Endotine, or Mitek or even cortical tunnels). Depressions do not occur if periosteum is not removed. Because the skin incisions are limited and performed at the non–hair-bearing areas, the incidence of alopecia is minimal to none. To date, there are no reports of skin necrosis. It is a lasting operation, with good results observed for more than 10 years.19 Complications associated with both techniques include hematoma; frontal nerve injury, which is usually temporary and a result of stretching rather than transaction; and inadequate amelioration of wrinkles because of incomplete muscle removal. Scalp necrosis and infections are rare in both approaches. Alopecia is more common after the open approach, although it can occur and cause patient concern even with the vertical incisions of the endoscopic approach. An inability to close the eyes because of excessive elevation is uncommon. When it happens, it is usually the result of a concomitant blepharoplasty with skin overresection. To prevent this complication in the open approach, the eyelid surgery should be performed after the coronal lift. This is not easy because of swelling of the eyelids. In the endoscopic approach, the eyelid operation comes first, followed by conservative forehead elevation. If upper eyelid ptosis is corrected at the same time, the eyes should be protected by night patching and a daily application of a steroid-containing drop solution, because the patient may temporarily be unable to close the eyes (22%).19 Overelevation of eyebrows is more commonly seen in the open approach. It has also been seen in the endoscopic approach when permanent fixation is used (i.e., miniplates, Endotine, Mitek). Overelevation results in a surprised look. The surgeon must be precise in the degree of elevation, aiming to obtain open and bright eyes instead. With experience, we have learned strategies to reduce or prevent unwanted results. For example, to avoid creating a sad look, the surgeon should pull less on the central forehead.2 To obtain a lasting eyebrow elevation, the galea should be sutured laterally to the deep temporalis fascia.20 If division of the periosteum is vital to elevate the eyebrows, leaving the periosteum intact will prevent depressions. Because it travels more superficially, the surgeon can avoid injuring the frontalis branch of the facial nerve by staying in the plane of the deep temporalis fascia. During closure, not only should the surgeon close the scalp in layers, but primary approximation of the galea is essential. The endoscopic approach is superior to the open approach. It is a physiological method that meets the objectives of facial rejuvenation of the upper face (Figs. 20.8 and 20.9). Fig. 20.8 Preoperative appearance (a) and postoperative results (b) of the standard endoscopic technique. Fig. 20.9 Preoperative appearance (a) and postoperative results (b) of the standard endoscopic forehead lift. 7 Passat R. La chirurgie esthetique des rides du visage. Presse Med 1919;27:258 8 Gleason MC. Brow lifting through a temporal scalp approach. Plast Reconstr Surg 1973;52(2):141–144 11 Sokol AB, Sokol TP. Transblepharoplasty brow suspension. Plast Reconstr Surg 1982;69(6):940–944 16 Paul MD. Subperiosteal transblepharoplasty forehead lift. Aesthetic Plast Surg 1996;20(2):129–134 20 Pitanguy I. Indications for and treatment of frontal and glabellar wrinkles in an analysis of 3,404 consecutive cases of rhytidectomy. Plast Reconstr Surg 1981;67(2):157–168
20
The Forehead Lift: Open and Endoscopic
Anatomy and Physiology of the Forehead Muscles
Elevator Muscle: Frontalis
Depressors: Procerus, Corrugators, and Portions of the Orbicularis Oculi
Eyebrows and Aging
Avoiding Unfavorable Results and Complications of Browlifts
Surgical Technique
Open


Disadvantages
Endoscopic

Advantages
Complications Common to Both Approaches
Conclusion
References
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


