The Eyelids
Upper Eyelid
Direct Closure
( Fig. 9.1 )
Direct closure is suitable for defects that involve up to one quarter (~8 mm) of the eyelid margin (semicircular flap closure, Fig. 9.1 ).
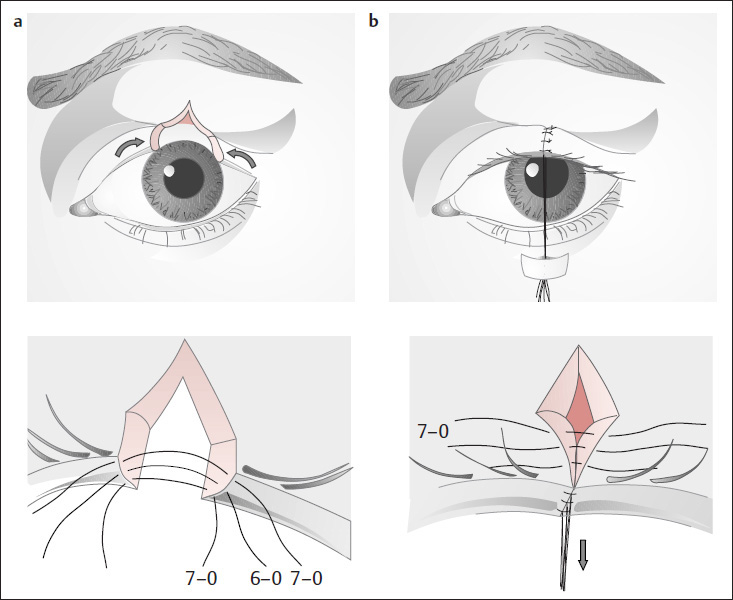
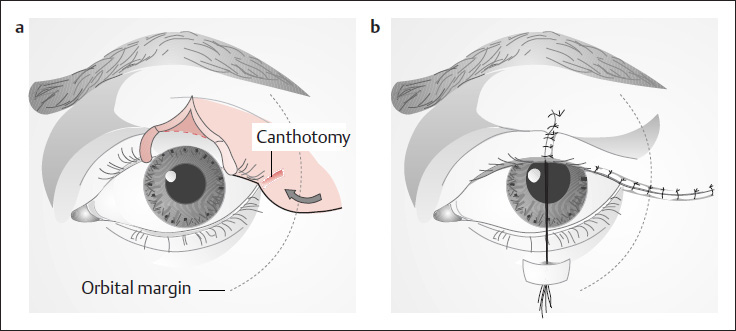
Semicircular Flap Closure of Beyer-Machule and Riedel (1993)
( Fig. 9.2 )
Larger defects involving up to one half of the lid margin can be closed by advancing a semicircular skin flap medially ( Fig. 9.2a ). The lid margin is sutured first ( Fig. 9.1 ). Next the tarsus and orbicularis muscle are approximated with 6-0 interrupted Vicryl sutures (Ethicon, Hamburg-Norderstedt, Germany), and the skin is closed with 7-0 interrupted monofilament sutures ( Fig. 9.1a, b ). The lid margin is approximated with three stay sutures, two of which are placed deeply (close to the eyeball) and one more superficially (Beyer-Machule and Riedel 1993). Large upper lid defects are rare and should be repaired only by surgeons who are experienced in eyelid surgery.
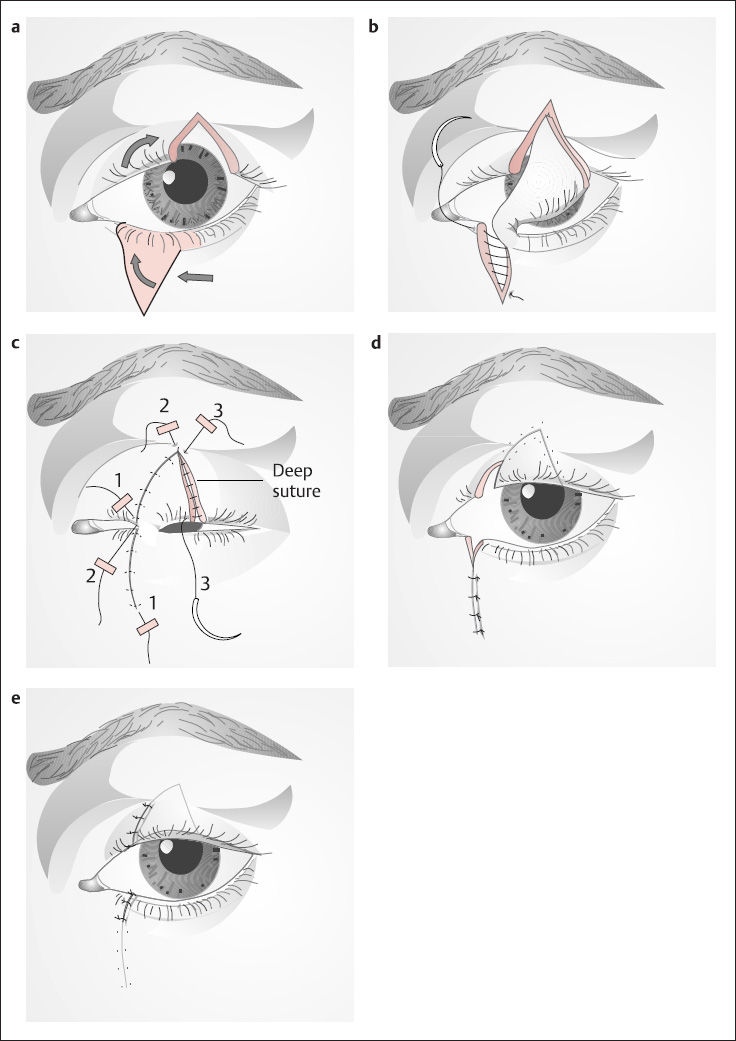
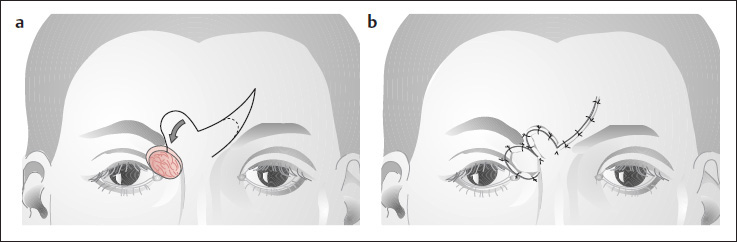
Switch Flap
( Fig. 9.3 )
Analogous to the Abbé lip switch, this flap can be rotated from the lower eyelid into a full-thickness upper eyelid defect involving up to one quarter of the length of the lid margin ( Fig. 9.3a, b ). The eye itself is covered with a special protector to prevent corneal injury. The lower lid defect is closed directly with continuous 6-0 monofilament ( Fig. 9.3b ), followed by placement of both the upper lid sutures ( Fig. 9.3c ).
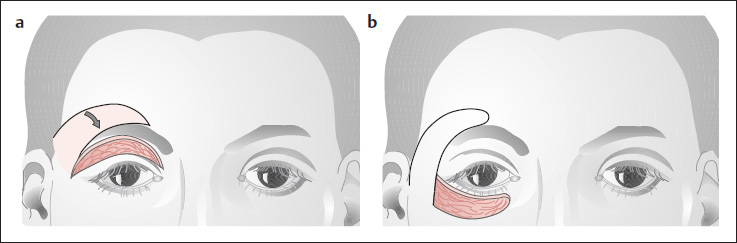
Upper Eyelid Reconstruction of Fricke and Kreibig
( Fig. 9.4 )
Large portions of the upper (and lower) eyelid can be reconstructed with a narrow transposition flap that is raised above the eyebrow on a lateral pedicle. Thick split retroauricular skin grafts can also be used.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


