The Cheek
Medial Cheek Defects
Upper Medial Cheek
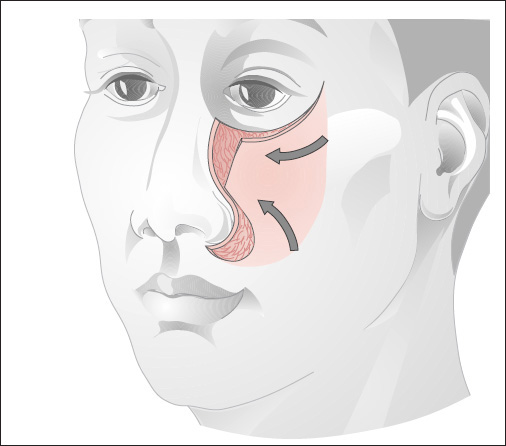
Esser Cheek Rotation (1918)
( Fig. 8.1 )
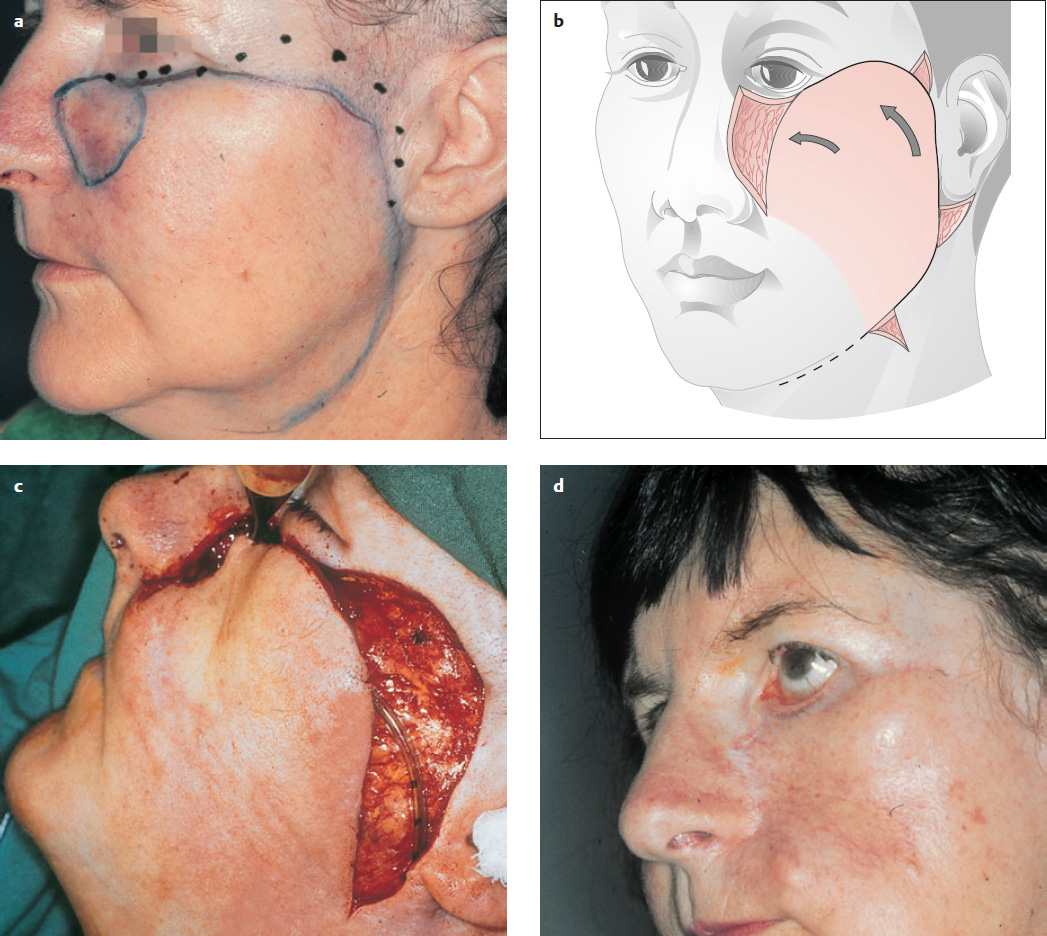
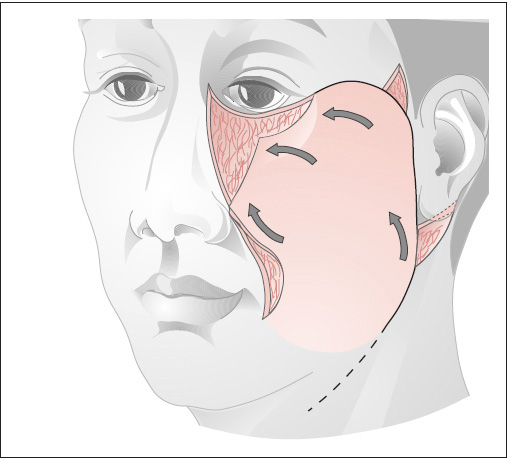
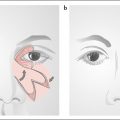
The Esser cheek rotation can be used to reconstruct portions of the nose, as well as the medial cheek (see also Fig. 5.52a ). From the defect, the incision extends along the lower eyelid and up into the temporal area, then curves down in front of the ear, where it may run a short distance back below the earlobe if necessary. It then proceeds downward and forward behind the mandibular angle ( Fig. 8.1 ). The circumscribed flap is mobilized in the fat plane and rotated forward. Ectropion is prevented by fixing the flap to the periosteum of the infraorbital region. Burow′s triangles are excised to close the secondary defect. If greater rotation is needed, the submandibular limb of the incision can be extended. The surgeon should not dissect too deeply in the fat, especially in the temporal area, as this could damage intact facial nerve branches.

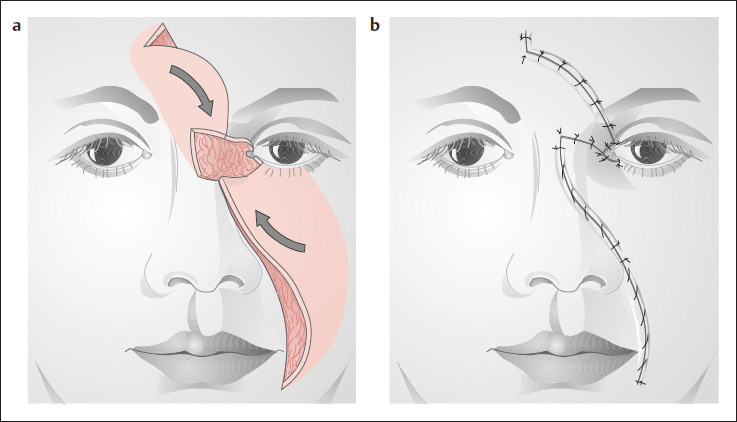
Cheek Reconstruction Combining the Methods of Esser (1918) and Imre (1928) (Weerda 1980)
( Fig. 8.2 )
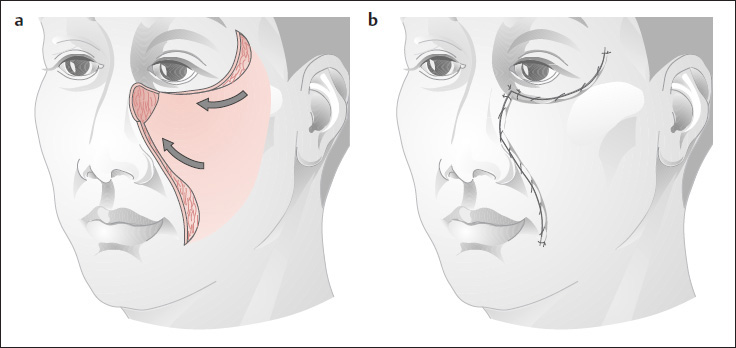
For defects of the medial cheek and lower eyelid area, it may be necessary to combine the Esser flap with a nasolabial advancement. We have obtained good overall cheek mobility by combining the Esser rotation with a two-layer crescent-shaped excision in the nasolabial fold.
Small Cheek Defects
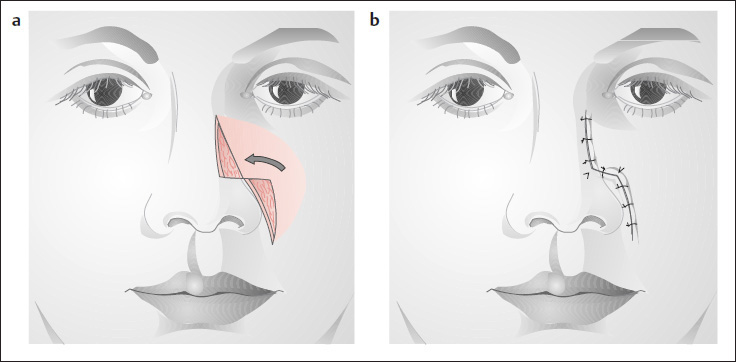
Small defects are repaired with transposition or rotation flaps, and small bilobed flaps can also be used (see pp. 21, 25, 46–48; Figs. 3.1b and 3.22 ). Defects in the nasal flank area can be closed by a Burow-type cheek advancement with a Burow’s triangle ( Fig. 8.3 ) or by excising a skin crescent in the nasolabial angle (see Fig. 8.4 ).
Defect in the Medial Canthus
( Fig. 8.6 )
A medial defect can be repaired with an Imre cheek rotation flap combined with a rotation flap from the forehead (see Figs. 5.2–5.8 ).
Mid-Anterior Cheek
( Fig. 8.7 )
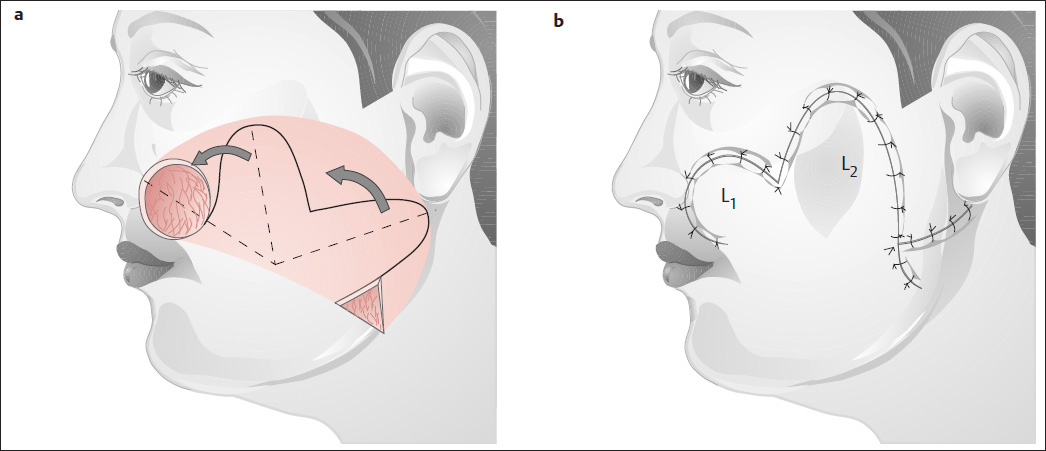
Pedicled Bilobed Flaps
Inferiorly based bilobed flaps are particularly suitable for elderly patients (Dean et al. 1975; Weerda 1983). The secondary lobe may be placed behind the ear or in the upper neck ( Fig. 8.7a, b ).
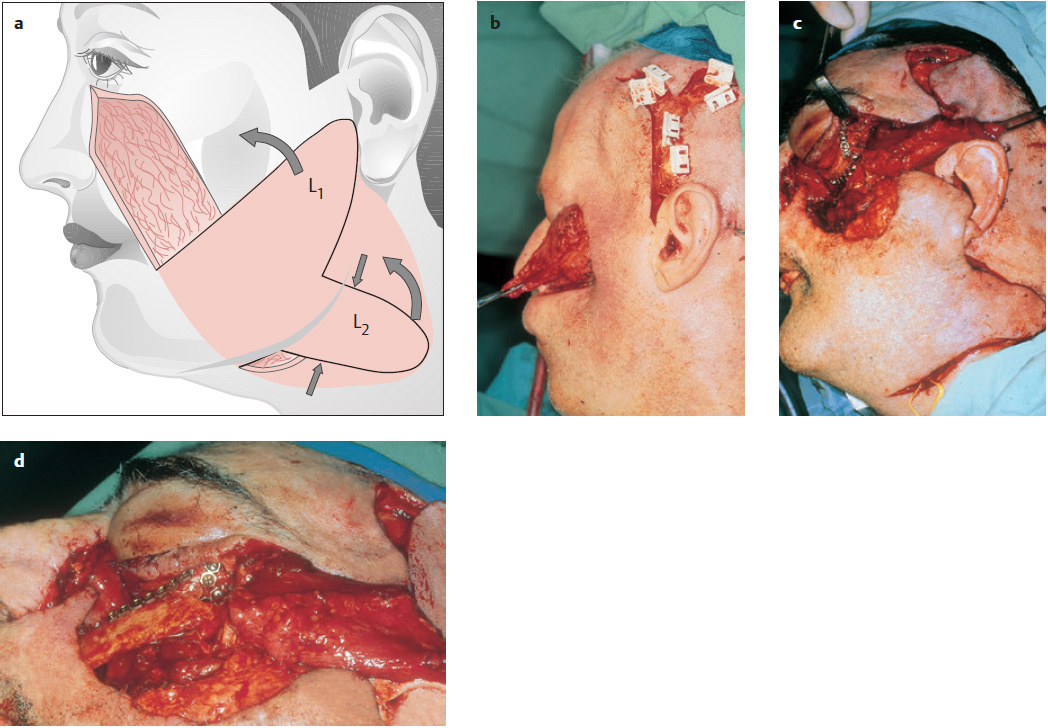
Large Inferiorly/Anteriorly Based Bilobed Flap
( Fig. 8.8 )
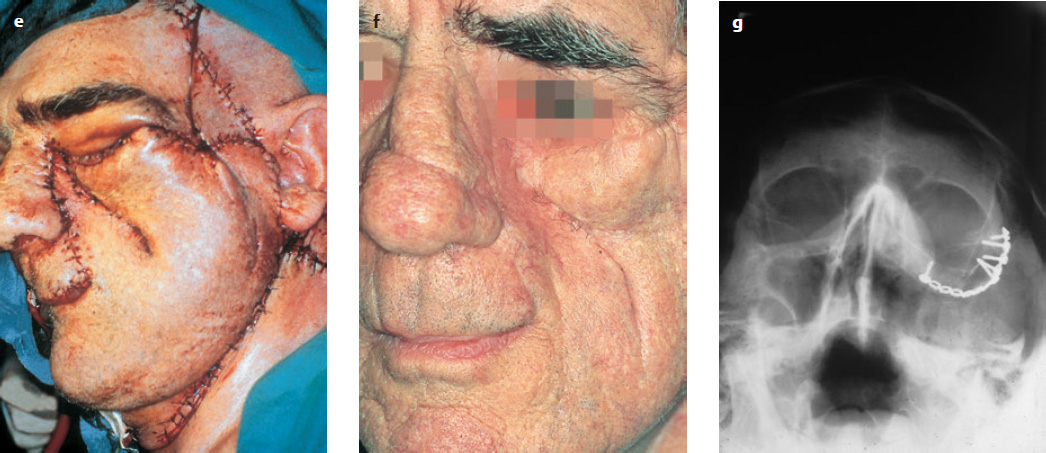
In modern oncosurgery, we normally reconstruct this defect with a free forearm flap (see Fig. 14.1 ). Sometimes, this bilobed flap can be used in older patients ( Fig. 8.8a ). The anterior sinus wall and orbital floor are reconstructed with temporal muscle and fascia ( Fig. 8.8b–e ).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


