CHAPTER 14 The Central Septum in Breast Reduction and Mastopexy

Key Points
Introduction
For a long time we have been used to seeing the breast as a homogeneous organ with unpredictable location of the neurovascular structures. In the course of numerous clinical breast reductions, nourished by the inferior pedicle1 I always came across a distinct layer of vascular networks. It emerged from the thoracic wall along the level of the fourth intercostal space and passed through the whole breast within the inferior pedicle to supply the nipple. The vascular layer was caudally attached to a horizontal septum of dense connective tissue.
Anatomical investigations showed that this septum is part of a suspension apparatus, which is attached to the thoracic wall, mainly following the borders of pectoralis major.2–4 This ligamentous suspension carries the whole weight of the breast like a sling. The horizontal septum takes its origin from the periosteum of the fifth rib and merges medially into a vertical medial ligament, which attaches to the sternum. Laterally, the septum merges into a lateral vertical ligament, which originates from the pectoral fascia at the lateral edge of pectoralis minor (Fig. 14.1). These vertical ligaments continue into the capsule of the breast in an anterior direction (Fig. 14.1). A ligamentous structure also arises from the origin of this deep part of the ligamentous suspension, which inserts into the overlying skin, thereby determining the shape of the breast. This structure can be seen as a densification of Cooper’s ligaments and builds the intermammary sulcus and the cleavage medially as well as the inframammary fold inferiorly. Laterally, it forms a strong ligament heading into the skin of the axilla, the suspensory ligament of the axilla, which shapes the axillary hollow.
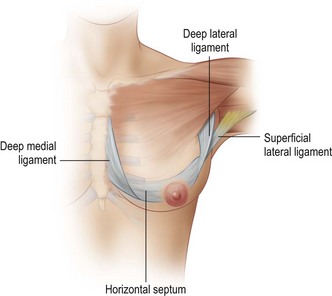
Fig. 14.1 Diagram of left breast, anteromedial view.
Redrawn from Würinger E, Mader N, Posch E, Holle J. Nerve and vessel supplying ligamentous suspension of the mammary gland. Plast Reconstr Surg 1998;101:1486–500.
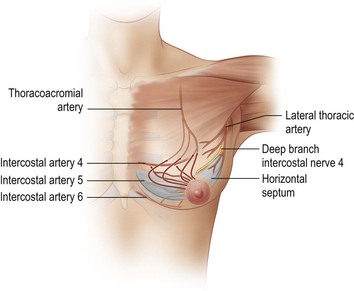
Most importantly, the deep branch of the lateral cutaneous branch of the fourth or fifth intercostal nerve (also the main nerve to the nipple), attaches to the caudal vascular layer (Fig. 14.2).
The second main path comprises perforating branches from anastomoses of the internal thoracic artery and the anterior cutaneous branches of the second to fourth intercostal nerves along the medial ligament as well as branches of the lateral thoracic artery and the corresponding lateral cutaneous nerve branches along the lateral ligament (Fig. 14.3).
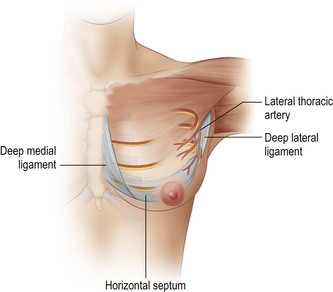
Fig. 14.3 Diagram of left breast, anteromedial view, neurovascular supply guided by vertical ligaments.
Redrawn from Würinger E, Mader N, Posch E, Holle J. Nerve and vessel supplying ligamentous suspension of the mammary gland. Plast Reconstr Surg 1998;101:1486–500.
The ligamentous suspension can be developed easily by blunt dissection along the retromammary space in a caudal direction. At the level of the fourth intercostal space the retromammary space changes its direction to continue as a horizontal plane of loose areolar tissue heading toward the nipple. This areolar tissue provides a pre-existing bipartition of the breast, as it divides the breast and its system of milk ducts into a cranial and a caudal glandular layer. Below this areolar tissue is the horizontal septum (Fig. 14.4).
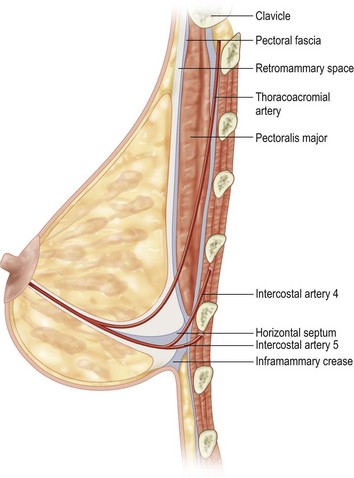
Fig. 14.4 Vertical sectional view.
The horizontal septum can be found by opening up the retromammary space in a caudal direction.
Redrawn from Würinger E, Mader N, Posch E, Holle J. Nerve and vessel supplying ligamentous suspension of the mammary gland. Plast Reconstr Surg 1998;101:1486–500.
The ability to localize the course of the neurovascular supply of the breast is important for any surgical treatment of this organ; it has allowed maintenance of the neurovascular supply in breast reduction procedures to be more precise.5–7
The nipple can be supplied by the vessels running along either of the vertical ligaments, merging into the subdermal plexus along the capsule of the breast, which affords a dermal pedicle to elevate the nipple. These pedicles can be cranial, medial, or lateral pedicles.8–10
The second big group of pedicles derives its neurovascular supply via the horizontal septum by a central parenchymal pedicle. These are the central and inferior pedicle techniques such as the techniques of Georgiade,1 Levet,11 Hester,12 or McKissock.13 Combining those two main neurovascular sources is possible.
Patient Selection
The technique could be offered to patients with large and ptotic breasts, to elderly patients, to smokers and obese patients, to pre-irradiated breasts, and to patients with weak connective tissue. Because of its safe neurovascular supply it can be applied to all these difficult cases. In secondary reduction the technique can be applied, when the horizontal septum was maintained previously.6
Indications
Related posts:
 Gluteal Flap Breast Reconstruction
Gluteal Flap Breast Reconstruction
 Surgery of the Breast in Poland’s Syndrome
Surgery of the Breast in Poland’s Syndrome
 Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
 Autologous Flap Use in Breast Reshaping after Massive Weight Loss
Autologous Flap Use in Breast Reshaping after Massive Weight Loss
 Fat Injections to the Breast: The Lipomodeling Technique
Fat Injections to the Breast: The Lipomodeling Technique
 Subfascial Breast Augmentation
Subfascial Breast Augmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


