Recognition of the brow as an integral contributor to periocular appearance improves and prolongs results from facial rejuvenation surgery. The approach to the brow and forehead in periocular rejuvenation must be chosen on an individual basis. The approaches discussed require in-depth knowledge of complex forehead and temporal anatomy to navigate the planes and important neurovascular structures safely. This article discusses anatomy, preoperative evaluation and considerations, surgical techniques, and complications in rejuvenation of forehead and brow.
The periorbital region is often the first facial area to manifest signs of aging. The eyes may appear heavy or tired long before an individual experiences jowling or frank rhytids. The delicate anatomy of the eyes and periocular area make it more amenable to showing the signs of aging. Youthful patients have a full or volumized appearance to their skin, with notable subcutaneous fat. The thin skin of the upper and lower eyelids is nearly anatomically devoid of this subcutaneous fat and thus has less of a buffer to the early signs of aging.
In the past, the periocular and brow regions were inadequately addressed in facial rejuvenation surgery. The effect that the brow and forehead have on periocular and upper facial aging has not always been a priority. Contemporary surgeons have come to realize that one cannot improve the appearance of the upper eyelid if the brow is ptotic and continues to encroach upon the upper eyelid. If brow ptosis is present and not addressed, the periocular region continues to look heavy with a fatigued appearance.
The forehead, invariably linked with brow ptosis, has additional contributions to the aged appearance. The receding hairline in men or a prominent forehead in both sexes has an effect on overall facial appearance. Kinetic forehead rhytids caused by the hypertrophic corrugator, procerus, or frontalis muscles are natural repercussions of human expression. All these 3 muscles may cause brow asymmetry.
The entire face, having been broken down into aesthetic units, merits a thorough evaluation of symmetry and substance, which vary individually with patients. What does not vary, however, is the interaction and dependence of adjacent aesthetic units.
Anatomy
The spatial position of an individual’s brow is affected by the relative contribution of brow elevator versus brow depressor muscles. The frontalis muscle is the only elevator of the brow. This muscle ends anatomically at the superior temporal line.
There are, however, multiple depressor muscles, including the procerus, corrugator, depressor supercilii, and orbicularis oculi muscles. The procerus muscle is responsible for the horizontal glabellar rhytids, and the corrugator muscle for the vertical glabellar rhytids. The frontalis muscle is contained within the galea, which is a tendinous sheet that also envelops the occipitalis muscle. The galea is relatively inelastic and extends laterally to join with the temporoparietal fascia. This transition occurs at the temporal line. Although physically separated at the zygoma, the temporoparietal fascia is anatomically congruent with the superficial muscular aponeurotic system in the lower face below the zygomatic arch.
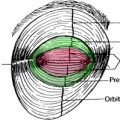
The orbicularis oculi is divided into 3 parts: preseptal, pretarsal, and orbital portions. This division is less of an anatomic designation and more of a functional division that aids the surgeon’s decision for therapy as well as serves as a surgical landmark. The pretarsal and preseptal components are self-explanatory, lying superficial to the tarsus and the orbital septum, respectively. These muscular subunits function somewhat involuntarily with blinking and are mechanical factors in the lacrimal pump system. The orbital portion of the orbicularis oculi functions in squinting and is more of a cause for dynamic rhytids, including the crow’s feet. This orbital portion is implicated in brow ptosis, medially and laterally.
The skin of the forehead is thick and is densely adhered to the underlying subcutaneous tissue. Deep to the subcutaneous tissue is the previously mentioned galea aponeurosis containing the frontalis muscles anteriorly and the occipitalis muscle posteriorly. The galea is separated from the periosteum by loose connective tissue. The periosteum is contiguous laterally with temporalis muscle fascia at the temporal line. The periosteum of the forehead has a confluence with the orbital septum at the superior orbital rim. This dense fascia condensation is called the arcus marginalis ( Fig. 1 ). It is imperative that these decussating fibers be released for adequate and enduring brow-lift results.