The Aging Face in Darker Racial Ethnic Groups
Pearl E. Grimes
Doris M. Hexsel
Marcio Rutowitsch
The aging face is an amalgam of many elements of time. It is a canvas of photodamage (extrinsic aging) and the imitable changes of time (intrinsic aging), including volumetric loss (fat atrophy) and gravitational soft-tissue movement. It is characterized by the appearance of coarse and fine wrinkles, skin laxity, jowls, mottled pigmentary changes, textural changes, redundancies, and loose skin. The aforementioned signs are unique to each individual, so that in aging, each person presents a greatly variable number of skin and soft-tissue alterations determined by genetic factors and environmental influences, such as sun exposure, smoking, and lifestyle.
Common signs of aging in fair-skinned patients result from photodamage as evidenced by wrinkles, skin laxity, dyschromia, and textural alterations; these tend to appear as early as the second and third decade of life. Darker racial ethnic groups have a higher content of epidermal melanin (see Chapter 2). In addition, fibroblasts are large and active, often giving rise to a thicker dermis. The photoprotective effects of melanin in darker racial ethnic groups retard many of the early telltale signs of aging, such as crow’s feet and periorbital wrinkles. Hence, photoaging changes are often minimized in deeply pigmented skin. Instead, soft tissue and gravitational changes may dominate cutaneous aging in darker skin types.
This chapter will review photodamage, intrinsic aging, and soft-tissue gravitational aspects of the intrinsic aging process in darker racial ethnic groups.
Photodamage
Photodamage results from the long-term deleterious effects of sun exposure. Clinically, photodamaged skin is characterized by coarse and fine wrinkling, mottled pigmentary changes, sallowness, textural roughness, and telangiectasias (Table 3-1). Histopathological features of photodamaged skin include significant epidermal and dermal alterations.1 The epidermal thickness may be increased or decreased, corresponding to areas of hyperplasia or atrophy. There is loss of polarity of epidermal cells and keratinocyte atypia. Dermal features include elastosis, degeneration of collagen, and anchoring fibrils. Blood vessels become dilated and twisted. Ultraviolet light exposure activates matrix-degrading metalloproteinase enzymes, including collagenase. Cytokines are released from keratinocytes. The cumulative effect is chronic dermal inflammation.2,3,4
Photoaging affects all races and skin types. Signs of photoaging may begin at an early age, as evidenced by freckles following ultraviolet light exposure. However, the clinical manifestations of photodamage may differ in lighter compared with darker skin types. In individuals with Fitzpatrick’s skin types I to III, or lighter-complexioned races, the clinical signs of photoaging—including wrinkles, laxity, dyschromia, and sallowness—may also be accompanied by an increased occurrence of premalignant and malignant skin lesions, including actinic keratoses, basal cell carcinoma, squamous cell carcinoma, and melanoma.
Glogau classified the severity of photodamage based on the extent of epidermal and dermal degenerative changes. Severity of photodamage is categorized from I through IV, ranging from mild to moderate to advanced or severely photodamaged skin (Table 3-2). The Glogau classification often facilitates the selection of appropriate treatment options in the aging Caucasian face.5 For instance, patients with mild photodamage often respond to topical anti-aging regimens and superficial resurfacing procedures, whereas patients who have moderate to severe photodamage require more aggressive resurfacing procedures or rhytidectomies.
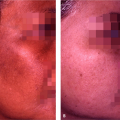
In deeply pigmented skin, photodamage may be characterized by mottled facial pigmentation, texturally rough skin, and fine wrinkles. In contrast to Glogau’s scale, advanced and severe photodamage are uncommon in deeply pigmented skin, in particular in African Americans (Fig. 3-2A–D). In a study by Grimes,6 100 women of color were surveyed regarding their concern about wrinkles, and the resulting data were compared with results from an age-matched population of 143 white women. Mean age of the white comparison group was 43 years. Sixty-five percent of the women of color—compared with only
20% of the white women—reported that their skin was not wrinkled. Only 2% of the women of color—compared with 20% of the white women—considered their skin moderately wrinkled. These results show a marked difference in perceived photoaging between women of color and white women. Montagna and Carlisle7 compared the morphology of facial skin of 19 black and 19 white women between the ages of 22 and 50 who had lived in Tucson, Arizona, for 2 or more years. Four-mm punch biopsies were taken from the malar eminence of each subject and processed for light and electron microscopy. These investigators reported that the stratum lucidum of black skin was not altered by ultraviolet light exposure. Black skin rarely showed areas of epidermal atrophy, and there was minimal evidence of elastosis. Overall, compared with white skin, black skin showed minimal evidence of photodamage. Two-mm punch biopsies of six women ages 45 to 50 with skin types V to VI from the Vitiligo and Pigmentation Institute corroborated Montagna’s findings.8 Biopsies were taken from the lateral periorbital region of each subject. There was no evidence of elastosis or epidermal atrophy. These women did, however, manifest mottled facial pigmentation and texturally rough skin, and in some instances, enlarged pores, which had worsened over time (Fig. 3-3A,B).
20% of the white women—reported that their skin was not wrinkled. Only 2% of the women of color—compared with 20% of the white women—considered their skin moderately wrinkled. These results show a marked difference in perceived photoaging between women of color and white women. Montagna and Carlisle7 compared the morphology of facial skin of 19 black and 19 white women between the ages of 22 and 50 who had lived in Tucson, Arizona, for 2 or more years. Four-mm punch biopsies were taken from the malar eminence of each subject and processed for light and electron microscopy. These investigators reported that the stratum lucidum of black skin was not altered by ultraviolet light exposure. Black skin rarely showed areas of epidermal atrophy, and there was minimal evidence of elastosis. Overall, compared with white skin, black skin showed minimal evidence of photodamage. Two-mm punch biopsies of six women ages 45 to 50 with skin types V to VI from the Vitiligo and Pigmentation Institute corroborated Montagna’s findings.8 Biopsies were taken from the lateral periorbital region of each subject. There was no evidence of elastosis or epidermal atrophy. These women did, however, manifest mottled facial pigmentation and texturally rough skin, and in some instances, enlarged pores, which had worsened over time (Fig. 3-3A,B).
Table 3-1 Clinical and histological features of intrinsic and extrinsic aging | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||
In contrast to the Montagna and Carlisle study, Whitmore and Sago9 measured the thickness of the epidermis and dermis on the non–sun-exposed forearm in 86 white women and 40 black women. They reported no statistically significant difference in skin thickness. Controlling for confounding variables—such as age, menopause, oral contraceptive use, hormone replacement therapy, cigarette smoking, and exercise—there was no relationship between race and skin thickness of black (1.39 ± 0.02 mm) and white (1.41 ± 0.01 mm) women. These findings suggest that the sun-exposed skin of whites is far more susceptible to the deleterious effects of ultraviolet light than is black skin.
The clinical features of photoaging in Asian skin differ from Caucasian skin. Asians tend to develop mottled pigmentation, solar lentigo, and seborrheic keratoses. In addition, Asians develop thicker, deeper wrinkles on the forehead, periorbital, and crow’s feet area compared with finer wrinkles in the aforementioned areas in Caucasians.10 Mild solar elastosis has been observed at 20 years of age in sun-exposed facial skin of Korean patients. Severe accumulation of elastotic material was evident in the dermis of Koreans older than 40 years of age. However, in sun-protected skin, solar elastosis was not present.11
Goh assessed photoaging in 1,500 Asians of skin types III and IV.12 The study included subjects of Indonesian,
Malaysian, and Chinese ancestry. Clinical manifestations of photodamage in this study included hypopigmentation, coarse and fine wrinkles, and tactile roughness.
Malaysian, and Chinese ancestry. Clinical manifestations of photodamage in this study included hypopigmentation, coarse and fine wrinkles, and tactile roughness.
Table 3-2 Glogau classification of the aging face | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
In a study of photodamage in 407 Koreans, standardized facial photographs were taken and evaluated by independent investigators to assess the severity of wrinkles and dyspigmentation.13 Wrinkling and pigmentation changes were a major feature of photoaging in Koreans. Women tended to have more severe wrinkles; seborrheic keratoses were the major pigmentary lesions in men, whereas hyperpigmented macules were prominent features in women. The number of hyperpigmented lesions and seborrheic keratoses increased with each decade of age. Cigarette smoking was an independent risk factor for wrinkles, but not for dyspigmentation, and caused additive detrimental effects to wrinkles induced by aging and sun exposure.
Toyoda and Morohashi14 assessed morphological alterations of epidermal melanocytes in photoaging in 15 Japanese women between the ages of 58 and 81. The investigators compared skin taken from the exposed crow’s feet area with the sun protected postauricular regions. Compared with sun-protected skin, the sun-exposed sites showed a statistically significant increase in melanocyte number, marked nuclear heterogeneity, and signs of cell activation. In addition, melanocytes were in close opposition to photodamaged, degenerated keratinocytes. Melanocytes in the sun-exposed areas also contained large intracytoplasmic vacuolar structures.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


