Introduction
The temporoparietal fascia flap (TPFF) is the thinnest, most pliable flap in the body, and can be used for moderate sized defects of up to 12 × 14 cm. The TPFF is highly vascularized and has a reliable arterial and venous pedicle. This flap’s greatest strength is in its versatility, as it may carry hair-bearing scalp, contain vascularized bone, or provide a thin covering for the ear or nose. The TPFF has gained greatest recognition for its utility as a pedicled flap for ear and nasal reconstruction and as a free flap in hand reconstruction.
This flap’s origins are evident in Monks and Brown’s reports of eyelid and ear reconstruction, as well as Fox and Edgerton’s description of the “fan flap” in 1976, which was used as an adjunct for ear reconstruction. Harii et al. first described the free scalp flap in 1974 as a free tissue transfer for hair transplantation ; however, the first free microvascular transfer of the TPFF was described by Smith in 1980. Further reports by Brent, Upton, and others pointed to the usefulness of this flap for coverage in the upper and lower extremities. In 1986, Abul-Hassan et al. examined the course of the superficial temporal artery and the middle temporal artery with its course through the deep temporal fascia. This work provided the anatomic basis for the development of a two-layered flap consisting of both the TPFF and deep temporal fascia. Since its original description, several refinements have been made to the TPFF that have included the incorporation of calvarial bone, temporalis muscle, and hair-bearing scalp. Most recently, endoscopy has been utilized for assistance in flap harvest. Though flap dimensions are relatively small compared with newer sources of vascularized fascia (i.e. lateral arm, serratus fascia, and anterior lateral thigh fascia) and dissection is at times tedious, the TPFF remains a valuable flap to have in one’s armamentarium. Perhaps the main advantage of the TPFF flap is that it leaves an almost inconspicuous donor site scar.
Flap Anatomy ( Figs 32.1 , 32.2 and see Figs 10.1 , 10.4 , and 10.5 )
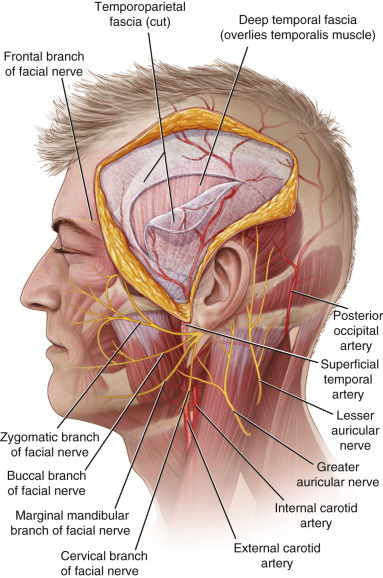
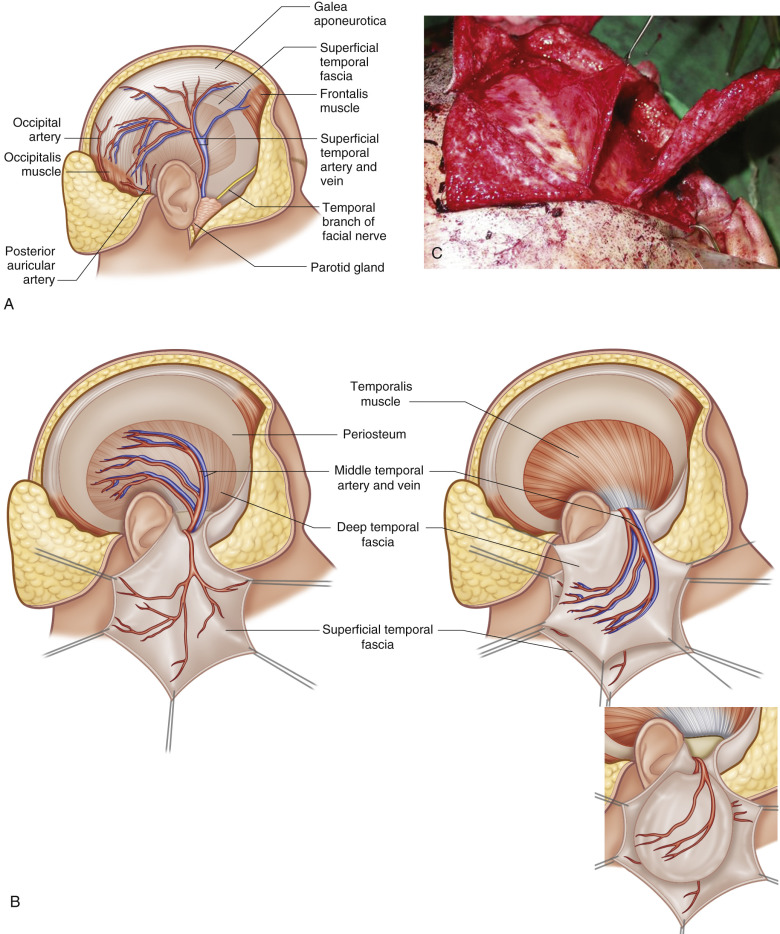
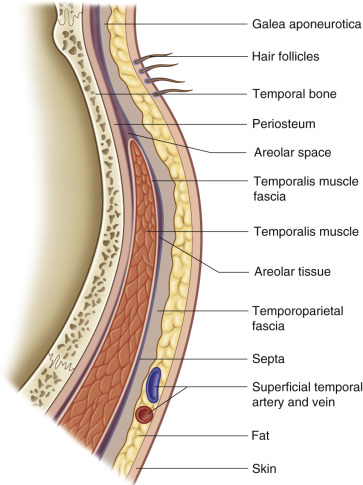
The temporoparietal fascia (TPF) is the cephalad extension of the superficial musculoaponeurotic system (SMAS) in the face. The TPF is located in the temporal fossa, which is bounded by the upper border of the zygoma, the supramastoid crest, and the superior and inferior temporal lines. The floor of the temporal fossa is composed of the temporal bone, parietal bone, frontal bone, and the greater wing of the sphenoid. The pterion is the junctional point of these bones. The scalp on top of the temporal fossa is itself a five-layered structure ( Fig. 32.3 ) (see also Ch. 10 , and Fig. 10.2 ) the skin and subcutaneous fat, which contains the hair follicles. Immediately beneath this fat is the TPF, which comprises the third layer of the scalp. At its superior margin, the TPF continues cephalad as the galea aponeurotics . Anteriorly, the TPF is continuous with the frontalis muscle and the occipitalis muscle posteriorly. Below the TPF lies a loose areolar plane that separates the TPF from the deep temporal fascia , which directly overlies the temporalis muscle; this areolar layer has been referred to as the innominate fascia . The deep temporal fascia continues superiorly over the temporalis muscle to become the periosteum overlying the temporal bone.
Arterial Supply of the Flap ( Figs 32.1 , 32.2 , 32.4 and Figs 10.4 , 10.5 )
Dominant:
superficial temporal artery
Length: 3.4 cm (range 2.5–5 cm)
Diameter: 2.2 mm (range 1.8–2.7 mm, at the level of the external auditory meatus)
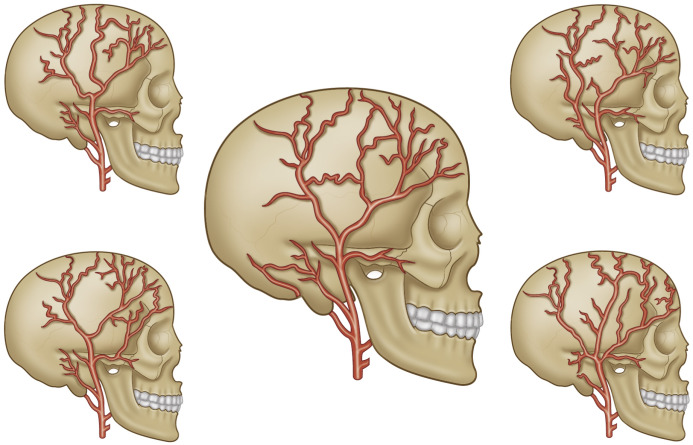
The TPFF flap is considered a Type A fasciocutaneous flap , with its direct cutaneous pedicle being the STA. Though many authors report the STA to be consistently present, Park et al. noted, in a study of 123 temporoparietal fascial flaps, that 88.2% of flaps were supplied by the STA, while 8.6% were supplied by the posterior auricular artery and 3.2% were supplied by the occipital artery. A higher percentage of arterial anomalies and hypoplastic superficial temporal arteries have been reported in patients with hemifacial microsomia, Romberg’s hemifacial atrophy and Treacher–Collins syndrome.
At the zygomatic arch, the STA enters the superficial temporal fascia. In 80% of cases, the STA bifurcates above the zygomatic arch into anterior and posterior branches (also known as frontal and parietal branches). In 5% of cases, a large middle branch also may be present. Terminally, the anterior branch of the STA supplies the frontalis muscle. The posterior branch of the STA connects with the branches of the occipital artery to supply the posterior scalp, while the central (or parietal) branch supplies the parietal scalp to the vertex.
The middle temporal artery arises from the STA, at or just superficial to the zygomatic arch. Immediately above the zygomatic arch, the middle temporal artery enters the deep temporal fascia. Harvesting the middle temporal artery with the STA allows for the construction of a vascularized bipedicled flap containing both the TPF and the deep temporal fascia ( Fig. 32.5 ).
Minor:
occipital artery
Length: 6.2 cm (range ± 3.5)
Diameter: 1.5 (range 0.6–2.0)
Identification of the occipital artery requires dissection through a posterior auricular scalp incision. The vessel arises posterior to the mastoid process and medial to the longissimus and splenius capitis muscles. The pedicle is identified underneath the semispinalis capitis muscle in a horizontal and oblique course. The vein is reported to be of similar caliber at this level though thin and friable.
Minor:
posterior auricular artery
Length: 6.4 cm (range ± 1.3 cm)
Diameter: 0.7–1.2 mm
The occipital and posterior auricular arteries are rarely used to supply the flap. If the STA is not available or the arc of rotation favors using these minor pedicles for reconstructing a defect, the flap can be based posteriorly on these vessels.
Venous Drainage of the Flap ( Fig. 32.2 and see Figs 10.4 , 10.5 )
Primary:
superficial temporal vein
Length: 3.4 cm (range 2.5–5 cm)
Diameter: 2.5 mm (range 2.1–3.3 mm, at the level of the external auditory meatus)
Secondary:
occipital vein
Length: 6 cm
Diameter: 1.2–2.0 mm
Secondary:
posterior auricular vein
Diameter: 2.4 mm
Venous drainage of the TPFF is through the superficial temporal vein in the majority of cases; however, venous drainage has been reported to be less consistent than arterial inflow patterns. In Park et al.’s study, only 63% of flaps were drained mainly by the superficial temporal vein, while the remainder were drained by the occipital or posterior auricular veins. The superficial temporal vein usually lies just anterior and superficial to the STA. However, it has been reported that the vein can be as far as 3 cm away from the artery. The vein runs with the STA to its origin, where the vein joins the maxillary vein to form the retromandibular vein, which drains into the external jugular vein.
Flap Innervation ( Fig. 32.6 and see Fig. 10.11 )
The auriculotemporal nerve (ATN) arises from the third division of the trigeminal nerve. It provides sensory innervation of the auricle, external meatus, tympanic membrane, temporomandibular joint, and temporal region. The nerve passes behind the condylar process of the mandible and then superiorly. At the level of the tragus, the ATN lies deep to the STA. The nerve then moves superficially to lie superficial to the STA at the level of the zygomatic arch. During dissection, the auricular temporal nerve lies posterior to the superficial temporal vessels and above the TPF and proceeds to innervate the temporal scalp. This nerve can be used to provide sensory innervation to the flap.
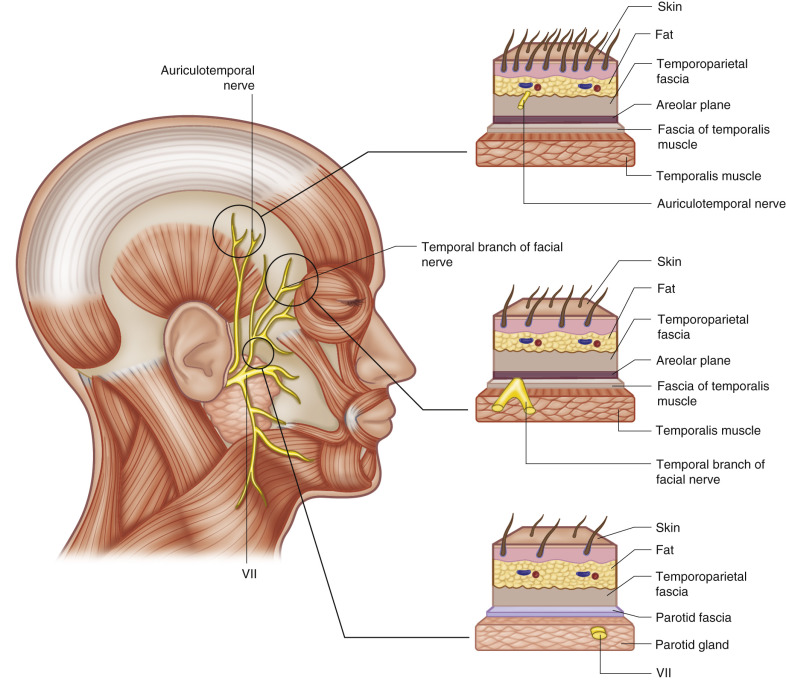
The zygomaticotemporal nerve also supplies sensation to the anterior temporal area of the scalp; however, this area is not routinely included in TPFF elevation due to its proximity to the temporal branch of the fascial nerve.
Flap Components
The flap may be transferred alone to provide vascularized fascial coverage. The flap may also include the overlying hair-bearing scalp, deep temporal fascia, temporalis muscle, and outer table of the temporal bone. Inclusion of the deep temporal fascia and temporalis muscle requires inclusion of the middle temporal artery during dissection. The auriculotemporal is included in the flap harvest and thus allows for the possibility of a sensate flap. The flap may also be raised as a bipedicled flap (bucket handle flap) in which both right and left TPF is harvested with inclusion of the right and left vascular pedicles.
Advantages
The TPFF has several positive attributes, the first being a relatively consistent arterial pedicle of large size (1.8–2.2 mm) and sufficient pedicle length (4 cm). Two teams may work simultaneously allowing for flap harvest and preparation of the recipient site. The flap is versatile and may be harvested as a composite flap with bone, in two layers, or split longitudinally in line with arterial branches. This flap may also provide a gliding surface for tendons. Most donor site incisions are unperceivable following hair growth. Finally, for auricular reconstruction, this flap has been shown to provide superior long-term results for contouring over cartilage grafts.
Disadvantages
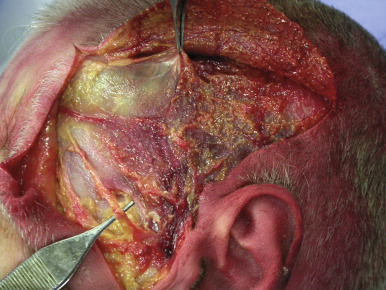
The major limitation of the TPFF is its limited size (12 × 14 cm), which makes the flap inadequate for larger reconstructive problems. Other disadvantages include the possibility of temporal nerve injury, alopecia, and the tediousness of the upper scalp dissection. Alopecia at the donor site is the result of damage to or destruction of the hair follicles within the thin scalp flaps elevated during flap harvest. Injury to the frontal branch of the facial nerve is possible ( Fig. 32.7 ). In some situations, the pedicle length of the TPF free flap may be too short to reach the recipient vessels and interpositional vein grafts may be required.
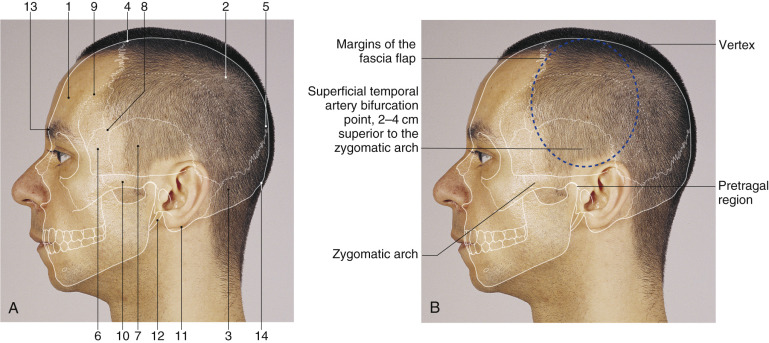
Flap Design ( Fig. 32.8 )
Anatomic Landmarks
The flap may be centered on a line running from the pre-tragal region to the vertex of the skull. The TPF is located over the temporal fossa extending from the zygomatic arch to the vertex. The STA is usually palpable just anterior to the tragus. The STA usually bifurcates 2–4 cm superior to the zygomatic arch, and may be identified with the handheld Doppler probe.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


