div class=”ChapterContextInformation”>
4. Psychological Techniques to Promote Adherence
Keywords
AdherenceComplianceDermatologyEducational interventionsIntentional nonadherenceUnintentional nonadherenceIntroduction
Providers often assume that the patient is capable of following a treatment regimen. However, research reveals this assumption to be erroneous. The lack of concordance between patient readiness and practitioner recommendations means that treatments are frequently offered to patients who are not ready to follow them. This reflects a bias towards treating the medical problem and underestimating the behavioral requirements of the treatment regimen.
Adherence is a complex behavioral process involving several interacting factors. These include characteristics of the patient, the patient’s environment (such as social supports, understanding of the health care system, functioning of the health care team, and accessibility to health care resources), and features of the disease in question and its treatment. Psychology offers useful theories, models, and strategies that supports evidence-based approaches to promoting adherence. Adherence interventions based on behavioral principles has been demonstrated in areas such as cancer, asthma, diabetes, and even sun-protection [1–4]. Psychological techniques can also be applied to health care providers and health care systems [5, 6].
This chapter describes several traits that are behavioral in nature and are also dynamic, and therefore amenable to intervention. We will discuss basic psychological principles of patients, health care providers, and health systems, and models of behavioral change that are relevant to adherence to treatment for dermatological conditions.
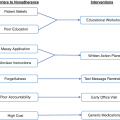
Patient-Centered Approaches
A patient’s attitudes, beliefs, and choices can prevent that patient from following treatment recommendations. Patient-based psychological approaches involve patients learning by association, such as developing self-management techniques, or learning how particular behaviors associate with a health outcome, such as cognitive behavioral therapy . Other techniques discussed in this section include adopting healthier coping-mechanisms, fostering self-efficacy, building self-awareness, and attending support groups.
Coping-Mechanisms
Coping mechanisms are psychological processes developed at a conscious level to manage difficult and stressful situations. The precipitation of adverse events and the subsequent coping mechanisms are known to mitigate adherent behaviour. For example, the consumption of alcohol may often be used as a coping mechanism for the patients dealing with distressing dermatologic disorders [7]. However, alcohol usage is associated with nonadherence in conditions such as atopic dermatitis, actinic keratosis, and acne [8–10]. In actinic keratosis, alcohol consumption negatively correlates with treatment satisfaction relating to the side effects of field therapy [9]. Furthermore, a study on subjects being treated for atopic dermatitis found that alcohol intake of greater than once a month was correlated with decreased adherence for oral medications, but not topical treatments [8].
Coping styles may be adaptive (meaning that the individual tries to reduce the stress) or maladaptive (meaning the individual keeps or even amplifies the current stressor). Examples of coping styles include: problem-focused coping, which includes planning, active approach, and deletion of concurrent activities; emotion-focused coping, which includes positive interpretation and growth, restraint, and acceptance; social support-focused coping, which includes the use of the social–instrumental support, the use of the social–emotional support, and the expression of feelings (venting of emotions); and avoidant coping, which includes denial and both mental and behavioral deactivation [11].
The relationship between different coping styles and dermatological patients has been explored in conditions such as melanoma, hidradenitis suppurativa (HS), and psoriasis [12–14]. Overall, patients with problem-focused coping had better adjustment to melanoma than those with passive or avoidant coping. Additionally, patients with problem-focused coping reported higher levels of self-esteem and vigor, fewer physical symptoms, and less anger and fatigue. In contrast, avoidance coping is associated with anxiety, depression, confusion, and mood disturbance in patients with early-stage melanoma [15]. Patients with HS utilized several coping and social support strategies, including positive reframing, humor, social-support, and avoidance [13]. Psoriasis patients who more frequently used normalizing/optimistic coping reported higher levels of mental health while those that used combined emotive coping strategies reported more disability, poorer mental health, and worse overall quality of life [14].
Although the relationship between coping mechanisms and adherence has not yet been explored for dermatological conditions, different coping mechanisms are associated with improved or worse adherence in other chronic diseases, such as chronic obstructive pulmonary disease (COPD) and diabetes mellitus [16, 17]. In a study of patients with COPD, the depression score was the highest in patients with avoidance-type coping and the lowest in patients with problem-focused coping (11.0 vs 5.6; P = 0.042), respectively, patients with social support-focused coping having the highest anxiety score in contrast to patients with emotion-focused coping, which had the lowest anxiety score (11.6 vs 5.0; P = 0.006) [16]. In diabetic patients, patients with emotion-focused coping had the highest level (P = 0.02) of diabetes-related self-care activities, followed by patients with social support-focused coping, and problem-focused coping, while patients with avoidance-focused coping had the lowest total score. Furthermore, patients with emotion-focused and social support-focused coping styles had increased adherence to diabetes-related self-care activities, while patients with other dominant coping styles were less interested in managing their disease [17].
In case of a multidisciplinary approach, identifying the coping styles in patients with chronic dermatological diseases represents an important aspect of the individualized treatment of the patient. While research suggests that people with more adaptive copying styles may have better adherence, it remains uncertain whether certain coping styles truly have a causal effect on adherence. For those with avoidant or social support-focused coping, psychological intervention such as cognitive behavior therapy may help support or change their coping style to more of a problem/emotional coping style.
Cognitive Behavioural Therapy
Cognitive behavioral therapy (CBT) is a psycho-social intervention that seeks to improve mental health by challenging and changing unhelpful cognitive thoughts and behaviors, improving emotional regulation, and developing coping strategies [18]. Another CBT that significantly impacts illness management is adherence enhancement, which focuses on fostering a collaborative therapeutic alliance that allows the patient to discuss problems related to treatment adherence. The therapist then determines if such problems are practical (e.g., financial challenges, inadequate education) or psychological (e.g., inadequate motivation, overwhelming stress, inaccurate beliefs, family beliefs), and then helps patients develop strategies that are tailored to increase the likelihood of adherence [19].
While CBT has been proposed to help acne patients manage proper treatment behaviors, it has most widely been studied in psoriasis patients [20]. CBT, including one-on-one, group-based, and online programs, is probably the most widely studied treatment with clear evidence of a positive effect on psoriasis activity, distress, and quality of life, especially if therapy is tailored to the individual [21–25]. In the online program, patients listened to simulated patients talk about common experiences and completed short assignments on self-esteem, thinking styles, coping skills, depression, and stress [24]. While online-CBT improved physical functioning (p = 0.03) and impact on daily activities (p = 0.04) compared to control, it did not improve psychological functioning (p = 0.32), up to 6 months after treatment compared to baseline. However, these studies highlight the promise of therapist-guided, individually tailored CBT to improve physical functioning and reduce the impact of psoriasis on daily activities in patients with a psychological risk profile [25]. Establishing a good therapeutic relationship may be an important factor that influences treatment outcomes in CBT interventions.
Self-Management
Self-management is a patient’s ability to manage symptoms, treatments, and physical and psychological consequences associated with a chronic condition. Since patients, not providers, are responsible for day-to-day disease management, patients must be more actively involved in their care through self-management. Evidence suggests that self-management interventions effectively increase patient knowledge, symptom management, and health status [26]. Self-management may help bridge the gap between patients’ needs and the ability of healthcare to meet those needs.
There is increasing interest in developing self-management interventions for patients [27–29]. Educational interventions teach parents to better understand the need for medical interventions and effective disease management. The content of educational interventions may include disease information, treatment instructions, management and prevention strategies. Approaches include pamphlets, workshops, programs, online video education, and Web-based interventions [30–33]. However, interventions solely based on education are unlikely to bring about health behavior change [33]. Real health behavior change occurs when health education and self-efficacy are combined so that patients are more comfortable with self-management .
Self-Efficacy
Self-efficacy is the extent to which a person believes they are able to successfully initiate and complete actions needed to achieve a specific outcome [34]. Self-efficacy influences how individuals approach goals, tasks, and challenges. Individuals with high self-efficacy tend to confront challenging tasks, while individuals with low self-efficacy tend to avoid challenges altogether [34]. Interventions that strengthen patient self-efficacy result in positive changes in health behaviors and improved health outcomes [28, 35, 36]. There are four key sources of self-efficacy: mastery, vicarious experience, verbal persuasion, and emotional regulation.
This approach has been applied to adult psoriasis patients with promising results. The intervention consisted of four components based on the four sources of self-efficacy : a nurse-led group learning experience, supporting written and audio-visual material, a follow-up telephone consultation, and a relaxation resource. While intervention participants had a modest reduction in psoriasis severity, there was insufficient power to detect significance.
Interventions to evaluate and promote parental self-efficacy have been applied to atopic dermatitis [27–29]. One such intervention was an eczema educational program, which involved measuring parental self-efficacy both before and after the program. The eczema program intervention was based on the self-efficacy construct and consisted of a nurse-led session designed to generate group interaction, provide opportunities for shared learning, and offer mutual support [37]. The intervention enhanced the self-efficacy score of participants, meaning increased self-efficacy in managing eczema and symptoms [28]. A web-based education program similarly increased the self-efficacy of mothers [27]. Further research into self-efficacy may help researchers plan patient education programs, measure the impact of patient education programs, and detect individual differences in self-efficacy between patients.
Self-Awareness
Patients may have limited control in their behavior, emotions , and thoughts in the pursuit of long-term goals. Appropriate medication usage may lead to decreased time for other tasks, thus decreasing a patient’s motivation for adherence. For example, a psoriasis patient may forgo using a topical medication because she has a social function and does not want the cream to show. Additionally, patients may have internal conflicts between prioritizing adhering to medication regimens with other responsibilities [38]. A mother may feel guilty spending time applying medication to her child with eczema and not spending time with her other children. Even if they are adhering to their medication, patients may still experience considerable distress, illness, and treatment uncertainty.
To aid self-regulation and promote adherence, patients are encouraged to reflect both on their beliefs about management of their illness and vital barriers that may be altering their adherence [39]. This approach may help patients identify potential solutions, help support psychological well-being, and enhance medication adherence. The identification and explicit recognition of potentially conflicting goals may itself be therapeutic and reduce distress. Increasing self-awareness of these conflicting goals may be therapeutic in itself by reducing expenditure of mental energy associated with internal conflict [40].
Patient Support Groups
There are many benefits to patient support groups . Support from peers may play a vital role in alleviating anxiety about the disease, improving health outcomes, and promoting medication adherence [41]. Studies demonstrate that peer support was associated with better outcomes among patients with chronic diseases [42]. Because psychological distress is frequently associated with skin disorders, support groups provide the social support, normalization of disease experience, and health literacy necessary to empower patients. Groups become valuable in normalizing a disease experience and conquering disease stigma, both of which have been found to cause nonadherence to medications in conditions such as psoriasis [38, 43]. In addition, increased health literacy through support groups help involve patients in the decision-making process for their disease management.
There is a growing trend to offer patient support programs to help patients and health care professionals better manage disease and optimize treatment. A study by the National Psoriasis Foundation found that patients in the US participating in patient support groups were more aware of treatment options, more likely to try more treatments, and were more satisfied with the treatment they were provided with [44]. Patient enrollment in the patient support group for those receiving treatment with adalimumab was associated with greater adherence, improved persistence, and reduced medical (all-cause and disease-related) and total health care costs [45].
Of course, the effectiveness of patient support groups depends on the content and support delivered at the sessions. A disparity in health literacy within various patient support groups has been noted and it has been suggested that coordinated efforts between organizations should be held to maximize the impact of patient group messaging [44]. Despite this, the empowerment that patients can get by being surrounded with others battling the same condition is a unique benefit all patient support groups can provide.
Physician-Centered Approaches
Because providers have such a significant role in adherence, designing interventions to influence their behaviour seems a reasonable strategy; however, few investigations on this subject have been reported in the literature. Physician-based strategies involve using motivational interviewing to help patients to better understand their behavior and its consequences, or helping learn by association, as discussed in the accountability section.
Motivational Interviewing
Motivational interviewing (MI) is a collaborative, patient-centered communications skill set that can increase behavior change by stimulating a patient’s own internal motivation for change. Medical providers using MI can explore factors associated with medication nonadherence, assess patient ambivalence and/or resistance, and educate a patient to promote medication-adherent behaviors. Core components of MI include partnership (e.g. collaborative care), compassion (e.g. empathy, acknowledgement of people’s thoughts/feelings), and evocation (e.g. eliciting patient-led solutions and management plans) [46]. The use of MI has expanded over the years from substance abuse to adherence to HIV-medications and more recently to adherence to other chronic medications [47]. Studies show that MI improves patients’ adherence to medication, even with different exposure times, different modes (in-office or over the phone), and different counselors’ background [48, 49].
MI has been explored in physicians treating psoriasis patients. A training program provided clinicians with MI skills to support behaviour change in patients with psoriasis and increase the clinicians’ knowledge of psoriasis comorbidities. The training enhanced clinicians’ ability to use MI skills to address behaviour change in the context of managing psoriasis and patient actors reported high levels of overall satisfaction with the consultation style used by clinicians following training. However, the clinicians’ knowledge of psoriasis-related comorbidities did not increase after training, nor were they more likely to explain to patients how psoriasis and behavioural factors are associated. The researchers suggested this may have been because the training focused less on the relationships between psoriasis-associated conditions and behaviours, and more on how to address behaviour change with patients [50].
Another study evaluated the effects of a 3-month individual MI intervention in patients with psoriasis with the aim of inducing behaviour change in daily psoriasis treatment. The MI intervention had positive overall effects on disease severity, self-efficacy, psoriasis knowledge, and health behaviour change compared to the control group. The researchers suggested that the MI may have enhanced the patients’ knowledge of psoriasis and reduced the risk of unhealthy lifestyle habits and nonadherence by encouraging healthy behaviours, facilitating the development of problem-solving skills, and providing emotional support and regular follow-up [51].
Addressing behavioural factors as part of psoriasis management is important because modification of lifestyle factors, medication adherence, and low mood can improve psoriasis outcomes and reduce the likelihood of developing or exacerbating psoriasis-related comorbidities. MI interventions to promote health behavior change can be tailored to individuals. MI can also change providers’ approaches to discussions with their patients on psoriasis management. Moreover, MI can be carried out within the context of a consultation about psoriasis.
Accountability
The accountability derived from the expectation of a social interaction between the patient and the health care provider may affect patients’ motivation to adhere to treatment. Accountability represents a potentially powerful tool to improve self-management, thereby promoting patients’ adherence to treatment. Accountability refers to the implicit or explicit expectation that an individual may be called upon to account for his or her actions or inactions [52]. Accountability requires social presence— which can be by telephone, by email, or in person—the latter of which is considered the most influential [53–55].
In previous studies, adherence in psoriasis patients to topical treatment dropped from 85% at Week 1 to 51% at Week 8 (p < 0.0001) [56]. However, there were increases in adherence around the times of the Day 7, 14, 28, and 56 follow-up visits. These office visits may increase patient motivation to adhere to treatment by imparting a sense of accountability. Other studies have also shown that early follow-up visits can at least temporarily improve adherence [57–60].
Digital interactions have also improved patient adherence to treatment. In a study of acne patients, weekly contact via an Internet-based contest substantially improved adherence to treatment [53]. The acne study included 20 male and female participants, aged 13–18 years, with mild-to-moderate acne who were prescribed topical treatment for 12 weeks. Participants were randomized 1:1 to a control group or to an Internet-based survey group to receive weekly emails with a link to a survey to assess their acne severity and treatment. The median adherence rate was 74% in the digital-intervention group and 32% in the control group. These findings suggest that having patients report how they are doing may be an intervention for improving adherence [53].
System-Centered Approaches
In addition to patient-centered and physician-centered behavioural techniques, internal modifications to clinical practices can create a facilitative foundation for adherence interventions. The functioning of the health system influences patients’ behavior in many ways. Systems direct providers’ schedules, dictate appointment lengths, allocate resources, set fee structures, and establish organizational priorities. Interventions in the health system are higher order interventions affecting health policy, organization, financing of care, and quality of care programs. System-based approaches discussed in this chapter include scheduling longer appointment times, continuity of care, and communication with patients.
Longer Appointment Times
The World Health Organization (WHO) recommendations for systemic actions to increase adherence include increased appointment lengths to allow enough time to address adherence [61]. Having more time to build rapport with a patient and communicate the importance of adherence becomes therapeutically valuable in the long-run.
In one study, subjects with psoriasis exhibited a negative exponential relationship between the duration of clinic visits and adherence. In patients who had a clinic visit that lasted less than 3 minutes, only 8.8% of patients were adherent to the physician’s recommendations. The percentage of adherent patients increased to 17.5% with a 3–5 minute visit, to 35.1% with a 5–10 minute visit, and to 28.1% with a visit lasting greater than 10 minutes [62]. Patients with a shorter visit were more likely to self-medicate, meaning they stopped using medications prescribed by doctors and instead sought other treatments. This suggested that good communication with doctors offered an important means to increase patients’ adherence, which has been well documented [63].
Continuity of Care
WHO also recommends for increased continuity of care, such as being followed by the same physician, to increase proper adherence, presumably through increased physician-patient rapport and accountability [61]. However, it may not always be feasible for patients to see a single physician for the duration of their disease. For example, dermatologic conditions may be diagnosed by a dermatologist and referred to the patient’s primary care provider for follow-up, or vice versa. In these cases, it may be useful to comment on the patient’s pattern of adherence, or any specific strategies the patient found helpful in increasing adherence in the referral notes to keep the patient accountable.
Communication with Patient
Ongoing communication efforts, such as phone calls, emails, or messaging through a patient portal, keep the patient engaged in health care [62]. This strategy is simple and cost-effective for improving adherence [64]. Additionally, communication with patients serves as a reminder for the patient to take their medication [65]. Furthermore, this ongoing support may help patients build rapport and feel more comfortable with self-management. However, consistent involvement may be considered overly intrusive for some patients, which makes informed consent an integral part of such reminder systems [66].
Conclusion
Interventions to promote adherence are not consistently implemented in practice. Providers report lack of time, lack of knowledge, lack of incentives, and lack of feedback on performance as barriers. Clearly, nonadherence is not simply a problem experienced by patients. From the first visit to the follow-ups, providers can assess risks for nonadherence and deliver interventions to optimize adherence. To make this a reality, providers must have access to specific training in adherence management. Furthermore, health systems must design and support delivery systems that develop this training. Providers can learn to assess the potential for nonadherence, and then use this information to implement brief interventions to encourage and support progress towards adherence.
Adherence is a problem observed in patients, but it has roots beyond the patient. Nonadherence occurs in the context of treatment-related demands the patient must attempt to handle. These demands include learning new behaviours, altering daily routines, tolerating discomforts and inconveniences, and persisting in doing so while trying to function effectively in their various life-roles. While there is no behavioral magic bullet, there is substantial evidence identifying effective strategies for changing behavior.
Behavioral interventions to promote adherence may provide immediate, practical strategies to improve patient adherence and therefore treatment outcomes for patients suffering from chronic dermatological conditions. A common goal of behavioral interventions is to increase patients’ involvement in care, thereby promoting better patient adherence. Improved self-efficacy and self-management enables patients may lead to better adherence, which leads to better health outcomes and reduced health care costs [67]. For dermatology patients to achieve fuller effects of medical therapies, providers need to better understand and more investigation into behavioral interventions to promote adherence.
Conflicts of Interest
Dr. Steven R. Feldman is a speaker for Taro. He is a consultant and speaker for Galderma, Abbvie, Celgene, Abbott Labs, Lilly, Janssen, Novartis Pharmaceuticals and Leo Pharma Inc. Dr. Feldman has received grants from Galderma, Janssen, Abbott Labs, Abbvie, Celgene, Taro, Sanofi, Celgene, Novartis Pharmaceuticals, Qurient, Pfizer Inc. and Anacor. He is a consultant for Advance Medical, Caremark, Gerson Lehrman Group, Guidepoint Global, Kikaku, Lilly, Merck & Co Inc., Mylan, Pfizer Inc., Qurient, Sanofi, Sienna, Sun Pharma, Suncare Research, Valeant, and Xenoport. Dr. Feldman is the founder, chief technology officer and holds stock in Causa Research. Dr. Feldman holds stock and is majority owner in Medical Quality Enhancement Corporation. He receives Royalties from UpToDate, Informa and Xlibris.
Dr. Adrian Pona, Dr. Abigail Cline, Dr. Masicampo, Monica Shah, and Felicia Tai have no conflicts of interest to disclose.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


