Techniques of Injections
Martin I. Boyer
I. Setup (Fig. 7.1)
All injections to the hand and wrist can be completed with the same formulation of local anesthetic and corticosteroid:
1 cc of 0.5% Marcaine
1 cc of 2% lidocaine
1 cc of 40 mg/mL of DepoMedrol
Other steroid or local anesthetic mixtures can be used if desired, but this is the preferred mixture of the author.
D. A 3 cc syringe is used, and a 30 gauge 0.5 in needle is utilized as well for all injections except those into the carpal tunnel. For those injections, a 25 gauge 1.5 in needle is used.
E. An iodine-impregnated swab stick is used for preparation of the injection site, and sterile gloves are utilized. A moist 4 × 4 gauze pad (either isopropyl alcohol or normal saline) is used to wipe out any blood or prep solution from the injection site, and a dry 4 × 4 gauze pad is used to clean the saline or alcohol. A band-aid is used to cover the injection site; it can be removed safely after a few hours.
II. Carpal Tunnel
A. Trans-FCR (Fig. 7.2)
The needle is introduced through the flexor carpi radialis (FCR) tendon, angled approximately 20 degrees in the frontal plane (aiming ulnarly) and 45 degrees in the sagittal plane. The needle is advanced slowly, taking care to redirect the needle should paresthesias be felt by the patient. The floor of the carpal tunnel is reached, and the needle is withdrawn slightly before injection is begun. A free flow of injectate should occur. Following completion of the injection, some patients may complain of persistent numbness in the median nerve distribution, although this is rare.
B. Carpal Tunnel: Ulnar Side (Fig. 7.3)
The needle is introduced at the wrist crease just ulnar to the palmaris longus tendon, angles approximately 30 degrees in the sagittal plane and no more than 20 degrees in the frontal plane (aiming radially). The needle is advanced slowly, taking care to redirect the needle if paresthesias are felt by the patient. The floor of the carpal tunnel is reached, and the needle is withdrawn slightly before injection is begun. A free flow of injectate should occur. Following completion of the injection, some patients may complain of persistent numbness in the median nerve distribution, although this is rare.
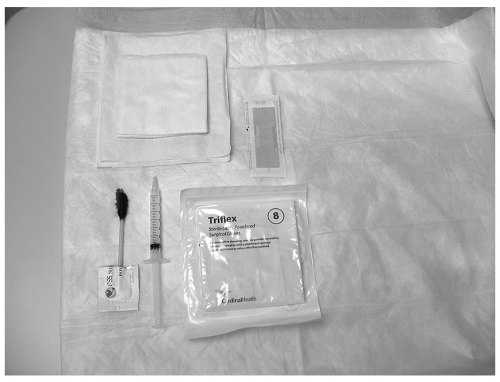 Figure 7.1 Setup. |
 Figure 7.2 Trans-FCR. |
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


