5 Suture Material
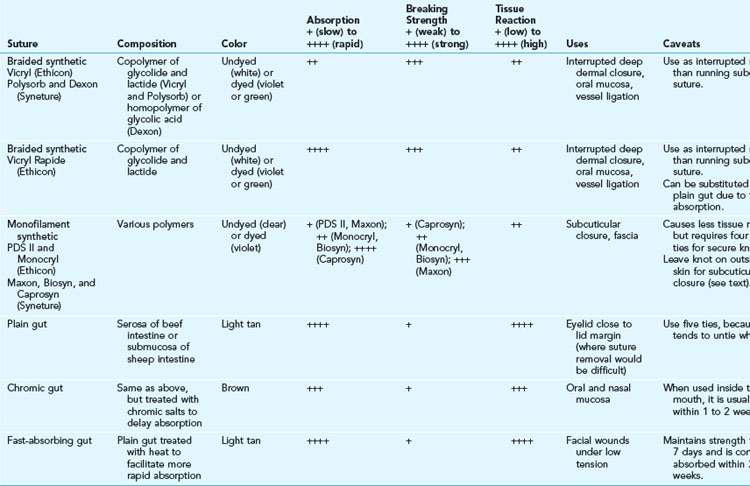
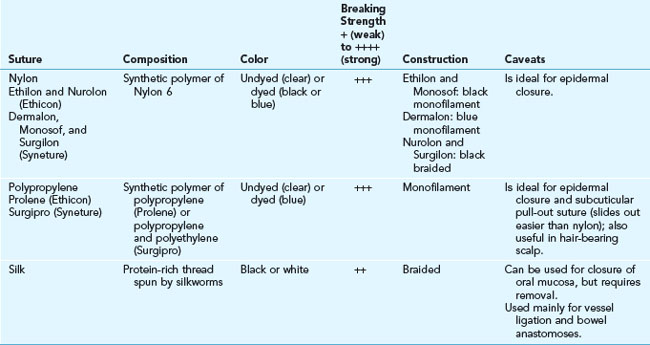
Many types of sutures are available, each with its own material properties, performance, and uses. The most useful sutures for skin surgery are described in detail in Tables 5-1 and 5-2.
History
The use of sutures to close wounds is certainly not limited to the modern era. Ancient civilizations developed innovative methods to close wounds based on the materials then available. Horsetail hair threaded onto eyed needles made from bone was utilized by the Greeks as early as 5000 to 3000 B.C. An Egyptian scroll dating back to 3000 B.C. describes the use of linen as suture material.1 South American Indians essentially created the first surgical “stapler” by using the heads of pincher ants to close wounds. The Roman physician Galen described the use of absorbable suture, specifically catgut, in 175 A.D.2 Sterile suture material was formally introduced by Lister in 1869 by treating catgut with chromic acid.3 Interestingly, the benefit of using sterile sutures was discovered during the American Civil War a few years earlier (1861–1865). Due to a lack of available suture material, Confederate surgeons were reduced to using horsetail hair, which they boiled to make more pliable. This inadvertent sterilization of the suture material most likely led to the lower wound infection rate they experienced as compared to their Union colleagues.4
Wound Healing and Sutures
Wound healing is described by tensile strength, the force per unit area required to pull a wound apart. Studies show that a wound does not begin to gain significant tensile strength until about 3 weeks after closure at which point it has only 10% of its final tensile strength. Tensile strength increases more quickly after 3 weeks and reaches its maximum strength at around 60 days. It never returns to more than 80% of normal skin.5 Thus, wounds subject to any tension should usually be closed in two layers: a deeper dermal layer with suture material that will maintain significant strength for 6 to 8 weeks, and a second superficial skin suture that can be removed in 7 days or less without fear of wound disruption. A suture or staple left in the skin for more than 10 days will often allow epithelial cells to grow from the surface down into the dermis along the suture or staple tract, resulting in permanent scar tissue on each side of the incision scar itself and detracting from the final appearance of the healed wound. In addition, a suture that is tied too tight will cause necrosis and subsequent scarring of the enclosed tissue within the loop, resulting in cross-hatch marks, or “railroad tracks.” The goal of the superficial suture layer is to carefully approximate the epidermis, not to add significant strength to the closure. The deeper dermal sutures should take nearly all tension off the epidermal closure.
Suture Material Properties
Suture material is judged by several characteristics:
Absorbability and Breaking Strength
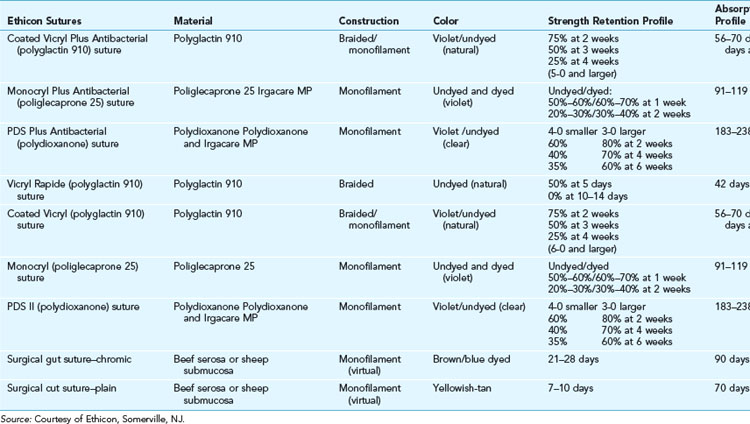
These terms are somewhat interrelated, as the absorbability of the suture correlates with the breaking strength of the suture with time. The United States Pharmacopeia (USP) officially defines absorbable sutures as those that lose breaking strength within 60 days, whereas nonabsorbable sutures retain their breaking strength beyond 60 days. See Table 5-3 for the details of strength retention and absorption in absorbable sutures. Breaking strength relates to the material used for construction of the suture as well as its diameter. The USP also defines the diameter of sutures. Sutures used for the skin usually range from 3-0 (relatively thick) to 6-0 (relatively thin). The smallest suture now available is 11-0 (about one-third the diameter of a human hair) and is utilized for the microsurgical repair of small blood vessels.
Absorbable Sutures
The absorbable sutures available in the United States are described in Table 5-1. Ethicon, a division of Johnson & Johnson, and Syneture, a division of Covidien, control 99% of the U.S. market (Ethicon, ~80%; Syneture, ~20%).6 Although absorbable suture is defined by its loss of strength within 60 days, the suture is not completely gone at that time. Even quickly absorbing sutures such as catgut can be found in the tissues for up to two years.7
Surgical Gut
Gut sutures have been used since 175 A.D. In addition to sutures, gut was also used for violin strings and bowstrings and, more recently, tennis racket strings. Gut sutures, also referred to as catgut, are derived from the intimal layer of the small intestines of sheep or cattle, and have nothing to do with cats. The origin of the name is unknown, but is thought to be derived from the word kitgut (fiddle string) with kit being the name of an Arabian fiddle with strings made from sheep intestine.8 Due to its heterogeneic derivation, it is highly inflammatory and is broken down quickly in vivo






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


