The Buccal fat pad may be addressed through both intraoral and extraoral approaches. This surgical guide will review the buccal fat pad, identify which patients may benefit from excision, and discuss current operative techniques.
Key points
- •
The buccal fat pad (BFP) contributes significantly to facial esthetics.
- •
The BFP can become problematic in young patients with round midfaces, congenital buccal lipodystrophy, or with esthetic disfigurement of the lower midface-jowl area.
- •
In the aging face, displacement of buccal fat or herniation secondary to weakness in the anterior SMAS can cause masculinization of the face.
- •
Buccal fat may be readily addressed through intraoral incisions or at the time of facelift (extraoral).
Video content accompanies this article at http://www.advancesincosmeticsurgery.com/ .
Introduction
The buccal fat pad (Bichat’s fat pad; BFP) is a well-defined, encapsulated triangular-shaped adipose mass in the cheek. It was first described by German anatomist Lorenz Heister in 1732 and later by French Anatomist Xavier Bichat in 1802. Although initially regarded as a nuisance factor that often would be incidentally encountered during facial surgery, it was later found to have clinical importance in the reconstruction of postsurgical oral defects [ , ].
The BFP was further detailed with the study of Gaughran and Tideman [ ], and more recently by Matarasso, Stuzin, Knize, and Geurrerosantos [ ]. Although initially the BFP held clinical importance in reconstructive surgery, elective BFP excision for face shaping and cosmetic reasons has become increasingly common in patients of all ages. Young patients, in large part due to social media, have recently become interested in facial shaping through BFP excision. Aging patients, seeking to restore a youthful appearance and redistribute facial fat can also benefit from this procedure [ , ].
The BFP plays a large role in the cheek prominence as well as in the suckling mechanism in newborns and infants. As growth of facial structure ensues, the volume of fat gradually diminishes. Despite this progressive atrophy with aging, it has been found to be hormone insensitive and unresponsive to weight fluctuations [ ]. Furthermore, because the BFP lies within a prominent position of the midface, it can contribute significantly to facial esthetics. In much of the population, there is an apparent decrease in size of the BFP in comparison to surrounding structures with aging. However, in individuals with persistent round midfaces, congenital buccal lipodystrophy, or with esthetic disfigurement of the lower midface-jowl area, the BFP can cause facial disharmony and excision may be recommended [ ].
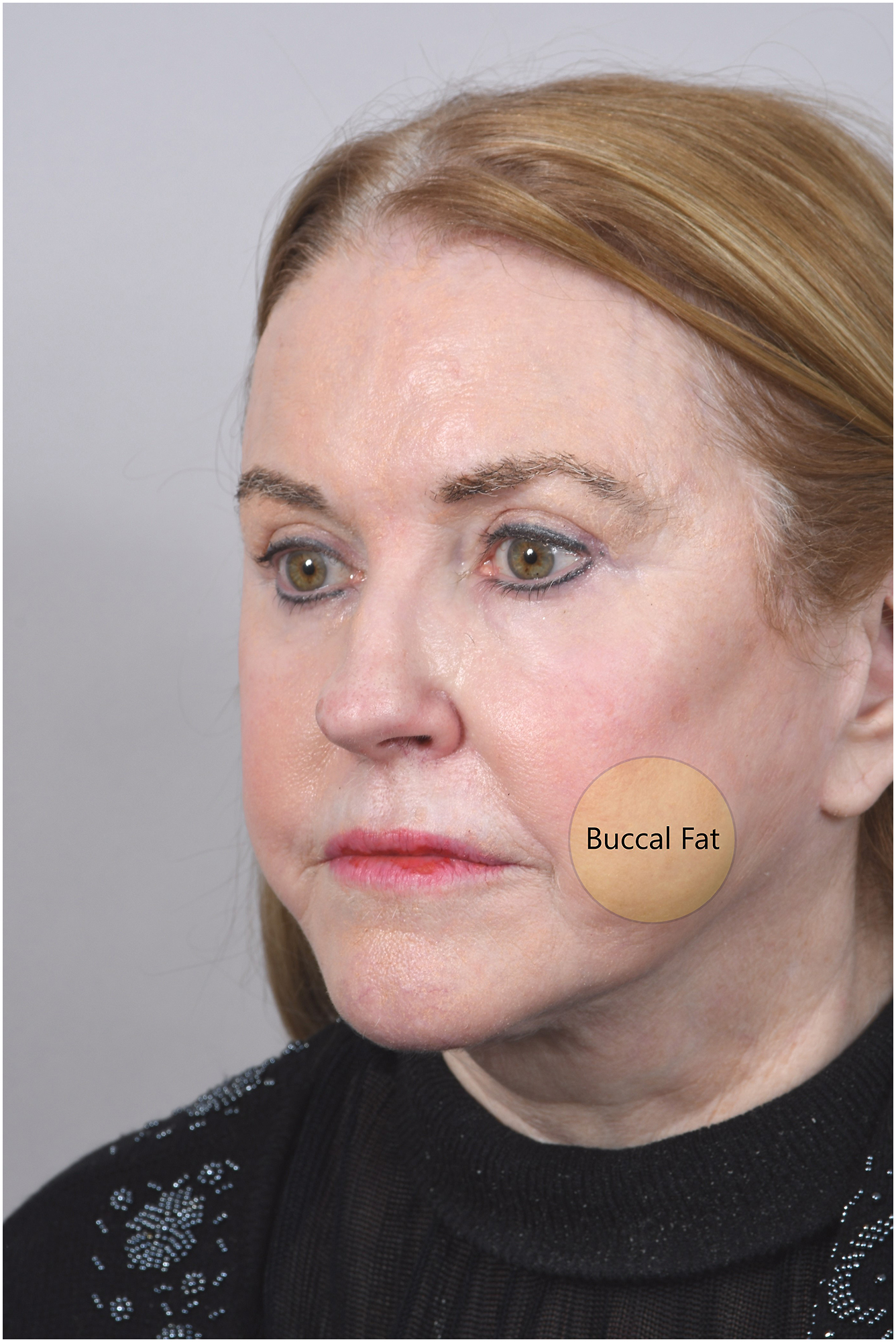
Masculinization of the female face with age is a common finding in the facelift patient population. The morphology of lower face aging is largely attributed to deflation of the midface and jowls coupled with skin laxity. As the facial fat begins to descend, the youthful triangle is lost and replaced with a squarer shape. In a small percentage of this population, a fullness is evident lateral to the jowl on physical examination, which has been observed clinically to be prominent BFP ( Fig. 1 ). Various possible etiologies of fullness lateral to the jowl have been described, including the following: (1) displacement of buccal fat [ ], (2) herniation of buccal fat secondary to weakness in the anterior superficial musculoaponeurotic system (SMAS) [ , ], or (3) a combination of both [ ]. In either case, pseudoherniation or displacement with prominence, buccal fat presents as a discrete reducible mass in the lower face lateral to the jowl [ , , ]. This pseudoherniation of BFP was first described by Stuzin in 1990 and later Guerrorosantos, Matarasso, and Knize, all of whom use an intraoral approach for the removal of this accessory cheek bulge [ , , , ]. Masculinization of the lower facial third drives patients to seek rejuvenation procedures, such as BFP removal [ , ].
Modern facial rejuvenation techniques aim to restore and reposition facial fat and volume [ ]. The ideal patient for isolated BFP excision has prominent zygomas that are poorly accentuated due to fullness within the cheeks. By removing the BFP, the malar eminence is highlighted and the cheekbones can appear stronger. BFP removal is contraindicated in patients with malar hypoplasia or thin cheeks because it will only serve to accentuate a cachectic or hollow appearance in these patients [ ]. Adults who seek reduction of fullness of the lower face to restore youthful esthetics are potential candidates for the excision of the BFP.
Social media exposure has also likely caused increasing rates of BFP excision in younger patients. However, there is insufficient evidence to support this as an effective or appropriate long-term solution in this patient population [ ].
Surgical technique (intraoral)
Preoperative planning
- •
History: Ascertain exactly which area of the face is problematic to the patient because often jowls or other areas of facial fat may be implicated in facial disharmony
- •
Physical examination: Examine patient in sitting position, and perform intraoral and extraoral palpations
- •
Counseling: No smoking 4 weeks prior and 4 weeks after, discontinue blood thinners, proper oral hygiene
- •
Set expectations: Explain that external changes will be subtle but overall facial harmony will be improved
- •
Photographs—4 views: frontal, oblique, right lateral, and left lateral
- •
Marking: The area of cheek fullness is marked in the preoperative area with the patient in sitting position ( Fig. 2 )

Fig. 2
The buccal extension of the buccal fat is marked preoperatively on the patient’s face.
Prep and patient positioning
- •
Supine positioning on operating table
- •
Standard oral RAE endotracheal tube should be used
- •
Prep with chlorhexidine gluconate mouthwash on a toothbrush or dilute betadine (wound class = contaminated)
Procedural approach (see [CR] , “intraoral approach to buccal fat removal”)
- •
The patient is induced under general anesthesia.
- •
A 1.5 cm intraoral incision is designed, oriented horizontally, and positioned 1 cm inferior and posterior to Stensen duct (identify the parotid duct opening at roughly the location of the second maxillary molar, Fig. 3 ).
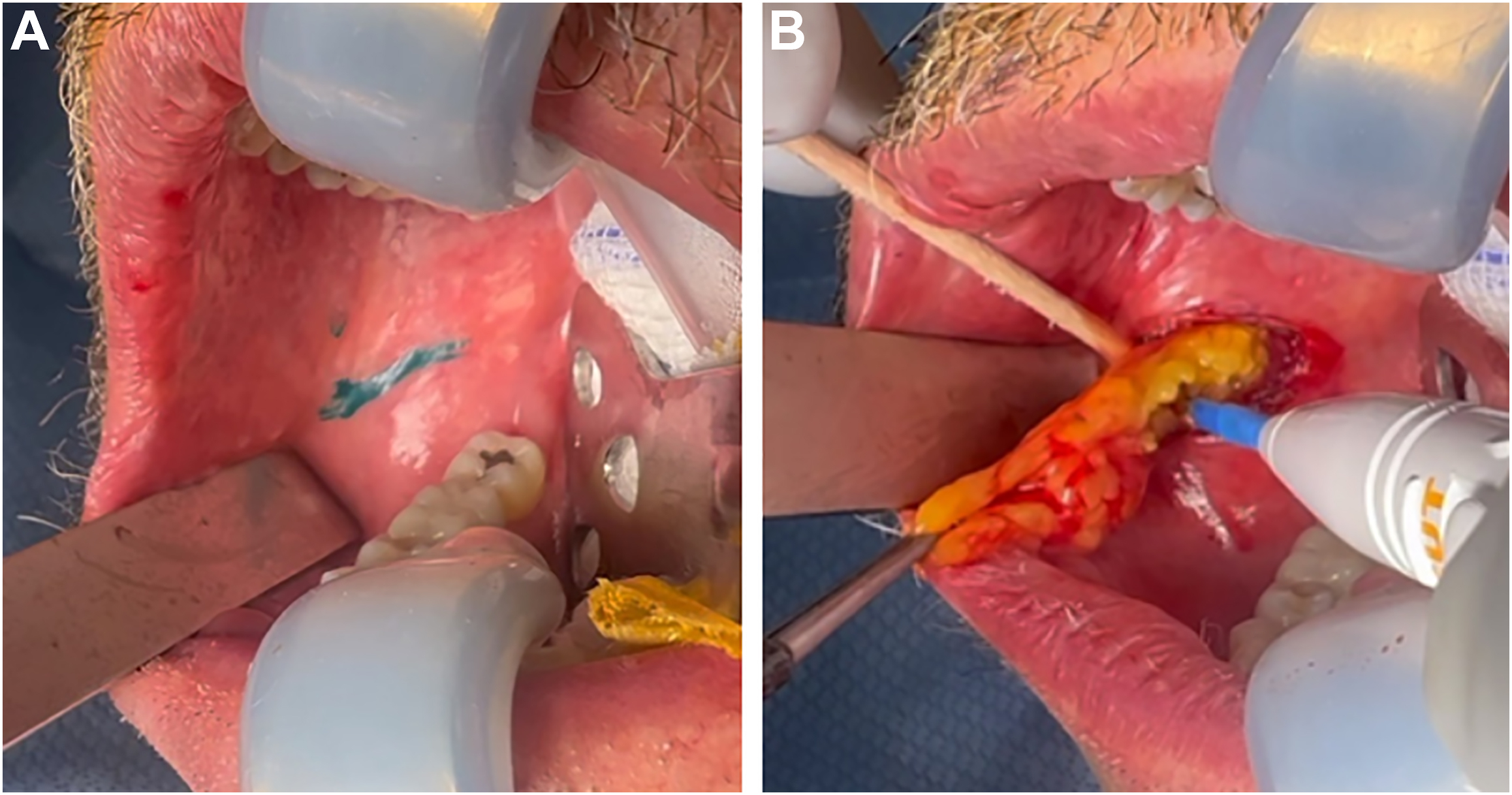
Fig. 3
( A ) Marking for incision, 1 cm below Stensen duct. ( B ) Intraoperative photograph during excision of buccal fat with unipolar electrocautery. Refer to [CR] for further description.
- •
The incision is injected with 1% lidocaine with epinephrine 1:200,000 mixed with tranexamic acid (TXA) (2 mg/100 cc of local anesthesia) and adequate time is allowed for the hemostatic effect of epinephrine.
- •
An incision is made with monopolar electrocautery through the mucosa and buccinator muscle.
- •
The BFP capsule is identified and bluntly entered using hemostat in the direction of the facial nerves (occasionally, external pressure on the skin over the BFP can help with intraoral identification).
- •
Hemostats are used to grasp and apply gentle traction to the visible fat. The fat is then transposed over a cotton-tipped application and resected with unipolar electrocautery, taking care to only resect such fat, which easily herniates into the surgical incision and can be resected under direct vision.
- •
Fat is removed incrementally to avoid overresection, with repeated external examination of the patient to determine end point.
- •
Meticulous hemostasis is obtained.
- •
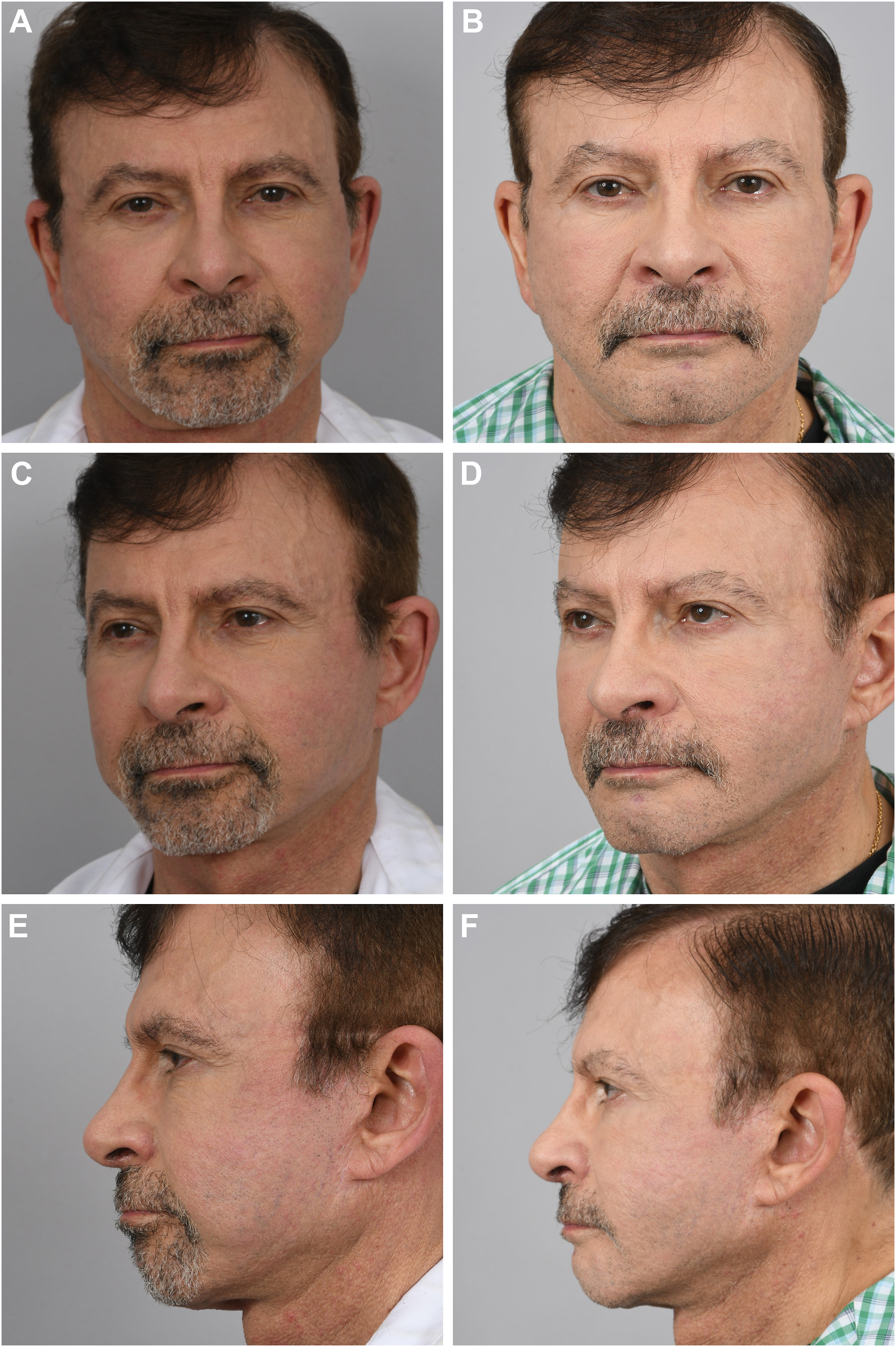
The fat is then weighed and compared to the contralateral side. The patient is evaluated for symmetry both in resection weight and in external appearance ( Fig. 4 ).

Fig. 4
This 75-year-old male patient is pictured after removal of the buccal fat with the corresponding fat transposed on the exterior of his face ( A ). Note the discrepancy of removed fat based on noted preoperative asymmetry, as well as the lobular appearance of the fat ( B ).
- •
The wound bed is irrigated and the incision is then closed with interrupted 4 to 0 absorbable sutures.
Immediate postprocedural care
- •
The patient is given chlorhexidine gluconate mouthwash and instructed to adhere to a soft diet for 24 hours with avoidance of very hot food, spicy foods, and fine particulate foods.
Postoperative results
- •
Refer to Fig. 5 below. This patient was extremely pleased with his result and did not experience any complications from surgery.