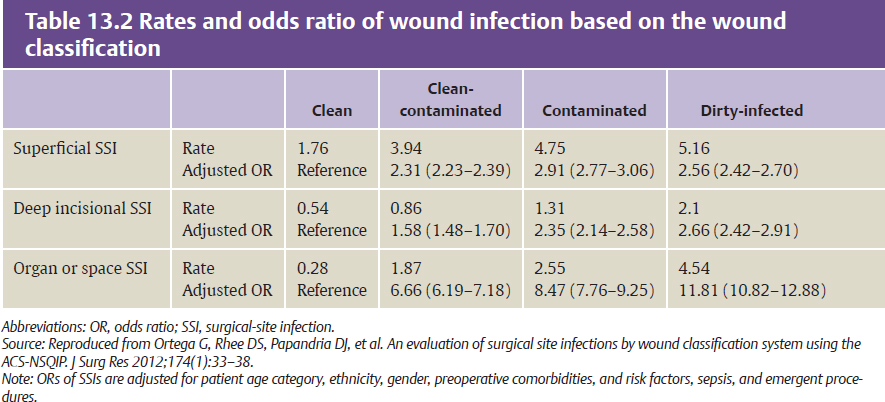
CHAPTER For centuries knowledge of infectious diseases rested on theories, which only recently have been replaced by the discoveries of science and the advances of technology. Until the development of bacteriology in the mid-19th century, the comprehension of infection in Western civilization was based on theoretical doctrines, and few preventive and therapeutic approaches had validity. Finally, near the end of the 20th century, scientific investigation augmented the understanding of infectious diseases by identifying hundreds of microorganisms and producing a diverse spectrum of antimicrobial agents for use in prophylactic and therapeutic regimens. Infection is defined as the product of the entrance, growth, metabolic activities, and pathophysiologic effect of microorganisms in the tissues of a patient. The normal biologic state of humans is not germ-free. Both transient and permanent flora resides on all skin and mucosal surfaces, all with the potential to cause infection. The absence of infection represents equilibrium between the factors of host resistance and the actions of bacteria. Clinical infection may result when this equilibrium is upset, by either an increase in bacterial inoculums or impairment in the host defense system. Surgical infections can be divided into two basic categories: infections requiring surgery and infections following surgery. Recognizing and minimizing the risk of surgical infection is crucial in minimizing patient morbidity and mortality. Multiple host factors have been shown to increase the risk of surgical infection (Box 13.1). Older age is a risk factor for surgical infection. Studies show that the risk of surgical infection increases by 1.1% every year between the ages of 17 and 65.1 Immune system senescence, among other factors, plays a role in increased infection risk. Hyperglycemia impairs the host immune system. Diabetic patients have an overall combined relative risk of 2.2 for surgical infection compared with nondiabetic patients.2 Obesity reflects overall poor health and is often associated with other factors that cause surgical infection, including hyperglycemia, malnutrition, and tissue ischemia. Studies have shown a stepwise increase in infection risk with increasing body mass index (BMI) (overweight BMI odds ratio [OR]: 1.6; obese BMI OR: 2.1; morbidly obese BMI OR: 2.5).3 Malnutrition is the lack of appropriate nutrients necessary to allow for appropriate synthetic function. This can be in the form of vitamin deficiency or caloric or protein deficiency. Low albumin (chronic malnutrition) and low prealbumin (acute malnutrition) is associated with a higher risk of wound infection after surgery. Vitamin deficiency, if suspected, should be treated to decrease the risk of infection. Early enteral feeding leading to improved nutrition in the first 48 hours has been shown to be clearly beneficial in reducing surgical infection risk (55% reduction in risk of surgical infection). • Older age • Malnutrition • Obesity • Diabetes mellitus/hyperglycemia • Prior site irradiation • Hypothermia • Hypoxia (at times secondary to hypoxemia) • Coexisting infection remote to surgical site • Immunosuppression (genetic, acquired [infection, malignancy, immunosuppressant medication, hypothermia, severe nutritional deficiency, hyperglycemia]) • Recent operation, especially of the chest or abdomen • Chronic inflammation • Nicotine use Nicotine causes direct microvascular vasoconstriction, and indirect pathways of vasoconstriction include the enhancement of thromboxane A2 and stimulation of cat-echolamine release. It also causes hypoxemia by decreasing oxygen carrying capacity (because of increased levels of carboxyhemoglobin) and is found to induce a prothrombotic state through multiple different pathways. Smoking was found to increase the risk of any type of surgical-site infection by an OR of 1.21.4 Patients with genetic alterations in their immune system or acquired alterations in their immune system (as a result of malignancy, infection, immunosuppressant agents, older age, malnutrition, or hypothermia, for example) are at increased risk for surgical infection. Tissue hypoxia predisposes to surgical infection. Tissue hypoxia can arise from hypoxemia caused by anemia, environmental toxins (i.e., carbon monoxide, methemoglobinemia), or pulmonary shunting (i.e., acute respiratory distress syndrome), among other causes. Tissue hypoxia can also arise from poor arterial inflow, as is the case in peripheral arterial disease, and can arise from direct tissue compression, or from compression of soft tissue impairing lymphatic or venous drainage, leading to edema, ischemia, and other conditions favorable to colonization and infection by microorganisms. Krizek et al5 quantified the effect of pressure on bacterial count, showing that incisions created in areas of applied pressure and inoculated with known concentrations of organisms allowed for a 100-fold greater bacterial growth than in areas not subjected to pressure. Numerous factors are involved in determining a patient’s risk for surgical-site infections. These are typically categorized as patient, environment, or treatment factors. All patient risk factors for infection are risk factors for surgical-site infection (see Box 13.1). In addition to those risk factors listed previously, an active remote infection at the time of an elective operation increases the risk for post operative wound infection. These infections typically arise from the urinary tract, skin, or respiratory tract. Also, studies show that methicillin-resistant Staphylococcus aureus (MRSA) carriers are 4.5 times more likely to develop surgical infections with MRSA than noncarriers. Carriers were divided into a control group and treatment group with mupirocin. Carriers treated with mupirocin had a significant reduction in the rate of surgical-site infection (3.7%) compared with the control group (5.9%).6 Environmental factors can increase the risk of surgical-site infection. Inadequate skin antisepsis has been shown to increase surgical-site infection. Studies comparing skin antiseptic agents have previously shown chlorhexidine-alcohol to be superior to all other skin antiseptics in preventing both superficial and deep surgical-site infections. However, subsequent studies have shown no statistically significant difference in skin antiseptic agents as long as one of the following is used: chlorhexidine, chlorhexidine in isopropyl alcohol, povidone-iodine, or iodine-povacrylex in isopropyl alcohol. Inadequate disinfection and sterilization techniques have also been implicated in causing increased risk of surgical-site infection. However, no convincing evidence has been found to prove that other environmental factors, including preoperative scrub technique, surgical glove damage, and barrier materials (e.g., caps, masks, shoe covers) correlate with postoperative rates of wound infections. Treatment risk factors have been associated with increased risk of surgical-site infections and can be divided into those that occur in the preoperative, intraoperative, or postoperative setting. In regards to preoperative hair removal, hair shaving doubles the risk of surgical-site infection when compared with hair clipping. The surgical site is an important factor in the assessment of surgical infection risk. Surgical sites are classified as clean, clean-contaminated, contaminated, or dirty-infected wounds according to the bacterial load of the wound7,8 (Table 13.1). The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) performed a study on the rates and OR of wound infection based on the wound classification9 (Table 13.2). Preoperative antibiotic prophylaxis can reduce the incidence of wound infection in selected cases. To be at an appropriate concentration at the operative site, a prophylactic antibiotic must be administered before an incision is made—preferably at least 1 hour before the procedure has begun. Several clinical trials and cohort studies have evaluated the efficacy of prophylactic antibiotics in plastic surgery. The decision to administer prophylactic preoperative antibiotics is not always obvious and requires that the risk factors for infection (i.e., dirty wound, devastating consequence to infection, prolonged operative time, implant use) be considered. The recommendations for antibiotic coverage are listed in Table 13.3.10 Table 13.1 Classification of surgical wounds
13
Surgical Infections
Risk Factors for Infection
Risk Factors for Surgical Infections
Risk Factors Specific to Surgical-Site Infections
Preoperative Infections
Clean | An uninfected operative wound in which no inflammation is encountered and the respiratory, alimentary, genital, or uninfected urinary tract is not entered. In addition, clean wounds are primarily closed and, if necessary, drained with closed drainage. Operative incisional wounds that follow nonpenetrating (blunt) trauma should be included in this category if they meet the criteria. |
Clean-contaminated | An operative wound in which the respiratory, alimentary, genital, or urinary tracts are entered under controlled conditions and without unusual contamination. Specifically, operations involving the biliary tract, appendix, vagina, and oropharynx are included in this category, provided no evidence of infection or major break in technique is encountered. |
Contaminated | Open, fresh, accidental wounds. In addition, operations with major breaks in sterile technique (e.g., open cardiac massage) or gross spillage from the gastrointestinal tract and incisions in which acute, nonpurulent inflammation is encountered are included in this category. |
Dirty-infected | Old traumatic wounds with retained devitalized tissue and those that involve existing clinical infection or perforated viscera. This definition suggests that the organisms causing postoperative infection were present in the operative field before the operation. |
Source: Reproduced from Simmons BP. CDC Guidelines on Infection Control. Infect Control 1982;3(2 suppl):187–196.
In clean, elective hand surgery, prophylactic antibiotic administration does not reduce the incidence of surgical-site infection in the outpatient population.11 However, antibiotic prophylaxis is recommended for patients who undergo elective surgery using K-wires or implants or who have a surgery that lasts longer than 2 hours. Also, those patients undergoing emergency hand surgery are recommended to receive antibiotic prophylaxis.12
Infections rarely complicate plastic surgical procedures to correct congenital anomalies. Postoperative wound infection or dehiscence after cleft lip and palate repair is reported to be as low as 1.3 to 4.3%. A prospective, randomized, double-blind study demonstrated no increased risk when cleft lip and palate repairs were performed without antibiotic prophylaxis.13 However, when performing ear reconstructions, studies support the use of prophylactic antibiotics, whether the support construct is formed of cartilage or alloplast, because of statistically higher rates of wound infection for auricular procedures than for procedures involving the rest of the face.13 If the surgical site involves the ear, an anti-Pseudomonas fluoroquinolone may be considered to cover Pseudomonas species.
Table 13.3 Prophylactic antibiotic recommendations for plastic surgery
Type of procedure | Recommended antibiotics | Alternative antibiotics |
Hand | ||
Clean Hardware placement Open reduction internal fixation | None Cefazolin Cefazolin | None Vancomycin Clindamycin or vancomycin |
Craniofacial | ||
Orthognathic (including cleft lip and palate) and mandibular, clean Orthognathic and mandibular, contaminated Hardware placement Septoplasty or rhinoplasty Ear reconstruction Ophthalmic Cancer-related surgery | None Cefazolin Cefazolin or cefuroxime Cefazolin Cefazolin + consider fluoroquinolone Topical neomycin–polymyxin B–gramicidin Cefazolin or cefuroxime + metronidazole or ampicillin–sulbactam | None Clindamycin Clindamycin Clindamycin Clindamycin + consider fluoroquinolone Fourth-generation topical fluoroquinolones (gatifloxacin or moxifloxacin): 1 drop every 5–15 min for 5 doses Clindamycin |
Aesthetic surgery | ||
Abdominoplasty, clean Skin, clean Skin, clean-contaminated | None None Cefazolin | None None Clindamycin |
Breast surgery | ||
Clean (augmentation, reduction, reconstruction) Implant placement Cancer-related surgery | Cefazolin Cefazolin Cefazolin | Clindamycin or vancomycin Clindamycin or vancomycin Clindamycin or vancomycin |
Microsurgery | ||
All flaps | Cefazolin | Clindamycin or vancomycin |
Source: Reproduced from Ariyan S, Martin J, Lal A, et al. Antibiotic prophylaxis for preventing surgical-site infection in plastic surgery: an evidence-based consensus conference statement from the American Association of Plastic Surgeons. Plast Reconstr Surg 2015;135:1723–1739.
The treatment of maxillofacial injuries, including facial fractures and laceration, incurs a moderate risk for infection, because the placement of hardware within dirty wounds is often required. In the treatment of open facial fractures, studies have demonstrated lower infection rates in groups treated with prophylactic antibiotics. Fractures within dirty skin wounds require prophylaxis for S. aureus and other cutaneous flora. Fractures communicating with the oral mucosa require prophylaxis for streptococci and the anaerobes Peptostreptococcus and Clostridium, which are common organisms of the oral flora.
Studies on septoplasty and rhinoplasty surgery showed an overall significant reduction in risk of surgical-site infection with antibiotic prophylaxis versus control (4.9% versus 11.%; OR 0.45; 95% CI 0.24 to 0.86; p = 0.02). Antibiotic prophylaxis significantly reduces the risk of surgical-site infection in patients undergoing contaminated septoplasty or rhinoplasty.10
In surgery for head and neck cancer, violation of the oropharynx appears to be a major risk factor for infection. Studies have demonstrated that infection rates are lower with the administration of antibiotic prophylaxis (5.8–38%) to patients undergoing tumor resection that violates the oropharynx versus placebo (24–78%) using a variety of regimens, including cefazolin, third-generation cephalosporins, and ampicillin plus cloxacillin.14–16 Antibiotics selected for prophylaxis or treatment in this patient population should provide coverage for S. aureus, Streptococcus, Peptostreptococcus, and gram-negative organisms.
Infections are relatively common after breast operations (1–30% of cases), because breast tissue has its own endogenous flora.17 As a consequence of communication with the external skin through lactiferous ducts, deep breast tissue contains a flora similar to that of normal breast skin.18 The organisms most commonly cultured from breast tissue include coagulase-negative Staphylococcus (53%), Propionibacterium acnes (30%), and diphtheroids or lactobacilli (9%).18 Antibiotic prophylaxis was found to prevent 38% of predicted infections in a prospective, randomized, multicenter study of 2,587 cases of reduction mammoplasties, lumpectomies, and mastectomies.19 A recent Cochrane review found prophylactic antibiotics beneficial in all procedures related to breast cancer.20 Also, antibiotic prophylaxis was found to significantly reduce the risk of surgical-site infection in patients undergoing cosmetic breast surgery.10
There are few studies evaluating antibiotic prophylaxis for aesthetic surgery. Studies have shown that for clean surgery of the skin, antibiotic prophylaxis did not significantly reduce surgical-site infection. Findings were similar for patients who underwent clean abdominoplasty. Therefore antibiotic prophylaxis is not recommended for patients who undergo clean abdominoplasty.10 At this time, it is unknown whether patients who undergo clean-contaminated skin operations need antibiotic prophylaxis.
There is a paucity of data addressing the use of preoperative antibiotics in free-flap reconstruction. Studies performed on patients undergoing oncologic head and neck reconstructive surgery and lower extremity reconstruction after traumatic injury show that preoperative antibiotics are effective in reducing surgical-site infections. Microsurgeons generally agree that this data should be extrapolated to all free-flap reconstructions and recommend preoperative antibiotic prophylaxis.21
Intraoperative Infections
Prolonged surgical time increases surgical-site infection risk, the rate of which doubles with each hour of surgery. Maintenance of intraoperative normothermia has a significant effect on the rates of wound infection. Patients with total intraoperative time (49 minutes) spent below 36° C developed more surgical-site infections (p = 0.04). One study showed a relative risk reduction of 57.7% in surgical-site infection when using systemic warming versus none.22
Glycemic control plays an important role in surgical patients’ outcome. Hyperglycemia interferes with healing and increases the infection rates and mortality in patients undergoing surgery. The risk of postoperative infections increases by 30% with every 40-point increase from normoglycemia (less than 110 mg/dL). Studies have shown chronic (Hgb A1C above 6.5%) and perioperative glucose levels (blood glucose levels higher than 200 mg/dL) were associated with an increased rate of dehiscence and infection.23 A statistically significant reduction in surgical-site infections has been seen with the use of higher intraoperative FiO2 levels. However, a subsequent Cochrane database systematic review of 28 randomized clinical trials including 7,597 participants compared a higher intraoperative FiO2 to a routine FiO2 and found it was not associated with a significant reduction in surgical-site infections and did not support the routine use of a high fraction of inspired oxygen during anesthesia and surgery.24
Studies have shown that surgical-site infections can be reduced by 20% with pulsatile lavage.25 High-pressure pulsatile lavage has been evaluated extensively in soft tissue contamination and shown to be seven times more effective in reducing bacterial load than bulb syringe lavage. The inherent elastic recoil of the soft tissues allows particulate matter to escape between pulses of fluid. The optimal pressure and pulse frequency seems to be 50 to 70 lb/in2 and 800 pulses/min. Adding antibiotics to lavage solutions, although commonly practiced, has not been shown to definitively improve outcomes.
Vacuum-assisted wound closure (VAC) optimizes blood flow, decreases edema, and aspirates accumulated fluid, thereby facilitating bacterial clearance. Therefore placement of a VAC device in the appropriate setting can be helpful in preventing surgical-site infection.
Postoperative Infections
Appropriate postoperative treatment can also decrease the risk of surgical-site infection. Despite good evidence for the use of antibiotic prophylaxis, antibiotic prophylaxis for more than 24 hours provides no advantage unless there is definite evidence of a wound infection. In some studies, use of antibiotics for longer than 24 to 48 hours has been shown to be harmful.26
The use of drains is controversial. Several studies have shown that drains placed in clean or clean-contaminated incisions have not shown a reduction in surgical-site infection. Prolonged drain use may pose an even higher risk; therefore they should be removed as soon as possible.27
Diagnosing and Managing Specific Infections
Summary Box
Common Surgical Infections
• Surgical wound infection
• Soft tissue infection
• Necrotizing fasciitis and gas gangrene
• Marine exposure
• Diabetic foot infections
• Osteomyelitis and septic arthritis
• Animal bites
• Snake, scorpion, and spider bites
Surgical Wound Infection
Although the risk of surgical-site infections is low, they comprise the largest portion (38%) of nosocomial infections. Anatomically, infections can be categorized as superficial, deep, or organ or space infection28 (Box 13.2). Depending on the location, they can present differently. Superficial infections present with the four signs of inflammation:
1. Calor
2. Dolor
3. Rubor
4. Tumor
or
1. Heat
2. Pain
3. Redness
4. Swelling
Deep infections have pus or an abscess with wound tenderness and fever. Deep infections can dehisce incision edges, exposing deeper tissues. Organ or space surgical-site infections occur within a body cavity and are directly related to the surgical procedure but may occur at the surgical site (mimicking incisional surgical-site infections) or at distant sites. Diagnosis of organ or space surgical-site infections requires postoperative imaging to confirm the site and extent of infection.
S. aureus causes many wound infections. The incubation period for S. aureus infection is 4 to 6 days. These infections tend to be localized with initial erythema, edema, pain, and eventual abscess formation. The pus is usually thick, creamy, white or yellow, and odorless. Spread to lymph nodes is unusual, but bacteremia is common. Fever and leukocytosis may be present. Furthermore, exotoxin release in S. aureus infection can lead to toxic shock syndrome, characterized by fever, rash, desquamation, involvement of three or more organ systems, and hypotension. Although treatment by opening the infected portion of the wound usually suffices, antibiotic therapy may be necessary when the infection is not well localized. A penicillinase-resistant penicillin or cephalosporin provides reliable S. aureus coverage. Given the higher incidence of MRSA, coverage for this must be considered, particularly in patients with a history of MRSA infection.
The number of wound infections caused by Staphylococcus epidermidis, which is a normal component of the skin flora, is increasing. The presence of this organism in wounds containing a foreign body (prostheses) is a reason for concern. A penicillinase-resistant penicillin or cephalosporin is required for adequate coverage of this organism, because strains resistant to penicillin are becoming increasingly common. If the infection involves a wound that contains a prosthesis, successful treatment may require removal of the prosthetic device. This is well described by the case presented in Fig. 13.1. The patient was managed according to the algorithm in Fig. 13.2 with appropriate antibiotic therapy and wound care before reconstruction.
Wound infections caused by gram-negative bacilli are increasing in frequency. Because the incubation period is 7 to 14 days, many patients are at home when the infection becomes evident. Infections caused by gram-negative organisms are associated with less erythema, edema, and pain than are staphylococcal infections. Instead of local inflammation, systemic signs, including fever or tachycardia, develop. Aminoglycosides and third-generation cephalosporins provide consistent gram-negative coverage, and quinolones are an acceptable alternative when oral administration is desired.
Infections with group A streptococci can run a fulminant course after initial presentation and diffuse cellulitis, lymphangitis, or lymphadenopathy. An area of rapidly advancing erythema with a raised, delineated border characterizes the cellulitis. Large, blood-filled blebs may form around the primary focus of infection, with the potential for local breakdown and progression to gangrene or necrotizing fasciitis if untreated (see discussion later in chapter). Streptococcal cellulitis usually responds to high doses of parenteral penicillin.
Infections caused by enterococci, S. faecalis, or other group D streptococci are less invasive than those caused by group A streptococci. Enterococcal infections are usually mixed, with enteric gram-negative organisms present. Thus enterococcal infections should be treated with ampicillin and aminoglycoside.
Soft Tissue Infections
Organisms that cause surgical-site infections are often the cause of surgical soft tissue infections. The two gram-positive cocci, S. aureus and Streptococcus pyogenes (group A), account for most skin and soft tissue infections. S. aureus invades skin and causes impetigo, folliculitis, cellulitis, and furuncles. Elaboration of toxins by S. aureus causes the lesions of bullous impetigo and staphylococcal scalded skin syndrome. The streptococci are secondary invaders of traumatic skin lesions and cause impetigo, erysipelas, cellulitis, and lymphangitis.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


