Surgical Correction of Panfacial Fractures
Detlev Erdmann
David B. Powers
DEFINITION
The facial skeleton is composed of four subunits: frontal, upper midface, lower midface, and mandible.
Panfacial fractures are defined as any fracture pattern that involves at least three of these four segments.1
ANATOMY
The face consists of 14 bones, 12 of which are paired (inferior nasal concha, lacrimal bones, nasal bones, maxillae, palatine bones, zygomatic bones) and 2 of which are not (mandible and vomer).
The frontal bone constitutes the major component of the forehead and forms the superior part of each orbital rim.
Zygomatic process of the frontal bone projects inferiorly to form the upper lateral orbital rim.
The zygomatic bone forms the lower lateral and part of the inferior orbital rim.
Malar surface: Convex shape, contains the zygomaticofacial foramen
Temporal surface: Concave, articulates with maxilla (articular surface) and contains the zygomaticotemporal foramen
Orbital surface: Contains the zygomatic orbital foramen
The nasal bones articulate with each other at midline as well as the frontal bone superiorly and the frontal process of the maxillary bone laterally.
Maxillae lie in between the orbit and the upper teeth and consist of a body, zygomatic process, frontal process, alveolar process (contains the teeth of the upper jaw), palatine process (forms 75% of the hard palate), infraorbital foramen, and maxillary sinus.
Forms the inferior and medial orbital rims
Articulates with the frontal, zygomatic, ethmoid, nasal, and lacrimal bones
The mandible consists of a body (anterior) and ramus (posterior).
The body of the mandible is further subdivided into the base and the alveolar portion, which contains the teeth of the lower jaw.
The ramus consists of two clinically significant superior projections:
The more posterior projection is called the condyle (which contributes to the formation of the temporomandibular joint).
The more anterior projection is called the coronoid process (which is the site of attachment for the temporalis muscle).
PATHOGENESIS
Facial fractures occur in the setting of trauma, with assault and motor vehicle collisions (MVC) as the most common etiologies (36% and 32%, respectively, of all facial fracture cases presenting to a representative US institution).1
MVC and gunshot wounds (GSW) have been specifically shown to be significant predictors of panfacial fracture patterns.1
PATIENT HISTORY AND PHYSICAL FINDINGS
Once the patient has been appropriately stabilized, obtaining as complete a history as possible is integral to assess for specific injury patterns even prior to performing imaging studies.
The following questions are most important when performing a systematic exam of the patient:
How and when did the accident occur?
What are the specifics of the injury?
What symptoms does the patient currently have (pain, altered sensorium, loss of consciousness, malocclusion)?
Certain subjective complaints can substantiate the presence of specific craniomaxillofacial injuries; for example, newonset anesthesia of the cheek/maxillary teeth may be a result of zygomaticomaxillary fractures resulting in injury of the infraorbital nerve.
Physical examination
Cranium/cranial base: Note any lacerations, swelling, ecchymoses, and contour irregularities.
Frontal region: Inspect for any lacerations, depressions, or crepitus.
Orbits: Examine for edema, ecchymoses, enophthalmos (possible zygomaticomaxillary complex fractures), emphysema, and limited upward gaze (possible inferior rectus muscle entrapment).
Nasal region: Check for signs of naso-orbital-ethmoid (NOE) fracture, such as septal deviation or hematoma and telecanthus.
Maxillary region: Assess for infraorbital nerve paresthesia or malar depression, trismus secondary to impingement on the coronoid process, and maxillary mobility.
Ear region: Examine for hematoma and integrity of auditory canal/tympanic membrane.
Mandible: Note the presence of external lacerations, ecchymosis or gingival tears (a possible sign of mandibular body or symphyseal fracture), step-off deformities, paresthesia along the distribution of the inferior alveolar nerve (an indication of fractures distal to mandibular foramen), periauricular pain, or malocclusions.
Additionally, a thorough intraoral, ocular, and neurological exam should be conducted to rule out dental malocclusions, ophthalmological emergencies, and focal neurological defects.
IMAGING
Computed tomography (CT) has largely replaced other imaging modalities as the standard for evaluation of facial trauma.
Axial, coronal, and sagittal cuts are utilized to visualize specific fracture patterns and reformatted to generate three-dimensional (3D) images (FIG 1A-C).
A standard head CT is better used as a screening tool, given its limited ability to visualize the zygomatic arch as well as the complete maxilla and mandible (FIG 1D,E).
A more complete craniomaxillofacial CT should extend from the vertex of the skull to the symphysis of the mandible.
3D CT imaging affords additional understanding of the spatial relationship of fracture fragments but does not provide information about soft tissue deformities.
NONOPERATIVE MANAGEMENT
Although most panfacial fractures are severe enough to warrant surgical treatment, facial fractures that are stable, nondisplaced, or asymptomatic may be managed conservatively with follow-up.2
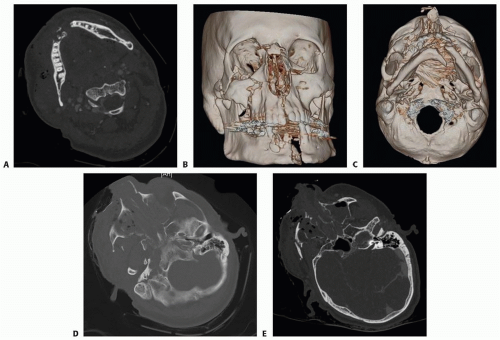 FIG 1 • A. Axial CT imaging can be used to visualize specific fracture patterns. B,C. CT imaging can be reformatted into three-dimensional images that are useful for preoperative planning. D. Craniomaxillofacial CT imaging provides a more comprehensive view of the zygomatic arch as well as the maxilla and mandible. E. Comminuted midface fractures. |
SURGICAL MANAGEMENT
The primary goal of panfacial trauma management is to establish an anatomically reduced platform from which to base the remainder of the reconstruction.
Preoperative Planning
Review of preoperative radiographs with 3D reconstruction is necessary.
Written sequencing of surgical approaches and goals for each section
Confirmation of necessary surgical instrumentation and plating hardware to reconstruct the defects
Positioning
The patient should be prepared and draped widely to allow for any and all needed exposures.
A horseshoe head frame may be used for coronal exposure.
Approach
One of the more common techniques for addressing midfacial fractures, often referred to as “outside-in” technique, focuses on first repairing the zygomatic arch to correct facial width.
Zygomaticomaxillary complex fractures are usually repaired with open reduction and internal fixation.3
The “bottom-to-top” approach focuses on reconstruction of the mandible first—generally accomplished as the
mandibular bone is less prone to comminution in most causes of panfacial trauma—which results in larger bone fragments that are technically easier to repair.
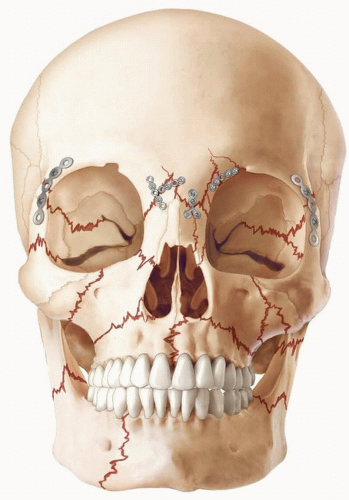
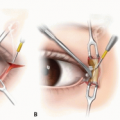
FIG 2 • The “outside-in” technique focuses on repairing the zygomatic arch first in order to correct facial width.
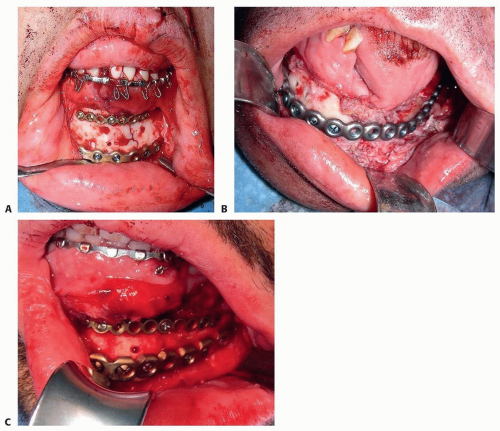
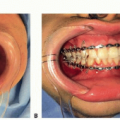
FIG 3 • Anterior (A), intraoral (B), and posterior (C) degloving incisions are made about 3 to 5 mm above the mucogingival junction and carried down through the mucosa, submucosa, facial muscles, and periosteum.
The “top-to-bottom” approach initiates repair at the forehead before working down to the maxilla and mandible (FIG 2).
The “bottom-to-top-to-middle” approach focuses on reconstruction of the mandible first—generally accomplished first because the mandibular bone is less prone to comminution in most etiologies of panfacial trauma—which results in larger bone fragments that are technically easier to repair.
Attention is then directed toward the zygomatic arches/frontal bar regions and the NOE/orbit, correcting any discrepancy at the Le Fort I level as the final intervention.
Possible incisions for gaining access to the mandible include the following:
Anterior degloving (FIG 3A)
Intraoral degloving (FIG 3B)
Posterior degloving (FIG 3C)
Hinds incision/posterior ramus approach (FIG 4)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree