CHAPTER 30 Superior Pedicle Extension Mastopexy
Key Points
Indications
Speaking generally, ptosis refers to relative descent of the NAC in relation to the breast mound with elongation of the distance between the nipple and suprasternal notch. The historical classification system used to define ptosis was elaborated by Regnault and defines three degrees of ptosis based on the relationship of the nipple to the inframammary fold (Fig. 30.1). A situation where the nipple lies at the level of the inframammary fold but above the level of glandular tissue is called first degree ptosis. In these cases, an augmentation mammaplasty is often adequate to correct the condition. In second degree ptosis, the nipple lies below the level of the submammary fold but above the lower contour of breast tissue. Third degree ptosis is characterized by a nipple located below the inframammary fold and at the lowest contour of the breast. Both second and third degree ptosis require some degree of skin reduction and tissue rearrangement for correction. Patients with this degree of ptosis are deemed appropriate mastopexy candidates. The condition of pseudoptosis is unique in that the nipple remains above the inframammary fold but the skin and glandular elements have fallen below the crease. This is usually corrected with augmentation.
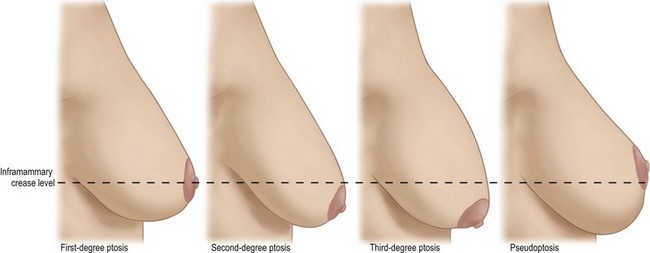
Fig. 30.1 Degrees of breast ptosis based on nipple position relative to inframammary crease.
Reprinted with permission from Boehm KA, Nahai F. Mastopexy. In: Nahabedian MY, editor. Cosmetic and reconstructive breast surgery, A volume in the Procedures in Reconstructive Surgery series. New York: Saunders; 2009.
Operative Techniques
Related posts:
 Saline Implants: Getting a Good Result
Saline Implants: Getting a Good Result
 Surgery of the Breast in Poland’s Syndrome
Surgery of the Breast in Poland’s Syndrome
 Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
 Autologous Flap Use in Breast Reshaping after Massive Weight Loss
Autologous Flap Use in Breast Reshaping after Massive Weight Loss
 Fat Injections to the Breast: The Lipomodeling Technique
Fat Injections to the Breast: The Lipomodeling Technique
 Subfascial Breast Augmentation
Subfascial Breast Augmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


