Structural and Physiologic Differences in the Skin of Darker Racial Ethnic Groups
Pearl E. Grimes
Quyn Sherrod
The color of skin is intriguing, for it evokes a multitude of societal emotions, interactions, inclusions, and exclusions. Descriptive terminologies for skin pigmentation are influenced by mythology, history, religion, anthropology, and geopolitical philosophies.1 Individuals with deeply pigmented skin comprise myriad racial and ethnic global populations. Skin color, among other defining physical traits, is the key determinant of race. According to John Hope Franklin, “…the specter of color and race haunts every nook and corner of the world, consuming an inordinate amount of mankind’s energies and attention that are so desperately needed to solve the major problems of peace and survival.”2
Humans (Homo sapiens) have been divided into five geographical groups as a basis for racial categorizations, including Caucasian, Mongoloid, Australoid, Congoid (or Negroid), and Capoid. Caucasoid includes Europeans, Middle Easterners, Pakistanis, and Indians. Mongoloid includes East Asians, Indonesians, Polynesians, Micronesians, American Indians, and Eskimos. Australoid includes the Australian Aborigines, Melanesians, and Papuans. Congoid includes Africans and descendants of Africans (African Americans and African Caribbean). Migration and consequent miscegenation make this historical system of classification somewhat obsolete. Recent studies have investigated genetic markers for categorization of racial ancestry. Genetic categorization clusters humans based on allelic heterogeneity and the resulting phenotypic differences.3 Variation in pigmentary phenotypes is attributed to the sequence diversity of the MC1R coding region.4
Ethnicity is a defined social construct based on national origin and phenotypic pigmentation (or skin color). Phrases commonly used when describing skin traits of darker racial ethnic groups include ethnic, dark, black, skin of color, and pigmented. The key unifying feature is skin with darker shades of pigmentation (tan, olive, brown, and black). Darker-skinned populations constitute the majority of the global population. They include Hispanics, Latinos, Africans, African Americans, Caribbeans, Native Americans, Pacific Islanders, East Indians, Pakistanis, Eskimos, Koreans, Chinese, Vietnamese, Filipinos, Japanese, Thai, Cambodians, Malaysians, Indonesians, and Aleuts.
In 2000, the United States Census Bureau estimated that the total resident population included 33 million Hispanic Americans (12%), 34 million African Americans (13%), 11 million Asians and Pacific Islanders (4%), and 2 million Native Americans, Eskimos, and Aleuts (1%). Statistical projections suggest continuing major growth of the nonwhite U.S. population, with Hispanics having the most significant growth rate. By 2050, at least 50% of Americans will represent darker racial ethnic groups.5
The popularity of cosmetic procedures is increasing substantially in the United States and globally. In the United States, patients are bombarded with cosmetic surgery images from television shows, newspapers, beauty magazines and books, the Internet, and infomercials. Media sources often present the most cutting-edge cosmetic procedures to the lay public. Patients today are more informed than ever.
All racial ethnic populations show keen interest in procedures to enhance one’s aesthetic appeal. Data from the American Society for Aesthetic and Plastic Surgery for 2005 revealed that the overall number of cosmetic surgical procedures increased 544% since 1997. The five most popular cosmetic surgical procedures in 2005 were liposuction, breast augmentation, blepharoplasty, rhinoplasty, and abdominoplasty. The top five nonsurgical cosmetic procedures were botulinum toxin injections, laser hair removal, hyaluronic acid filler injections, and chemical peels. Darker racial ethnic groups accounted for 20% of all cosmetic surgery procedures. Hispanics accounted for 9% of this group, African Americans 6%, Asians 4%, and other groups 1%.6
Cosmetic procedures commonly performed in darker racial ethnic groups include chemical peels, microdermabrasion, injectable fillers, laser hair removal, botulinum toxin injections, liposuction, and breast augmentation. Nonablative resurfacing procedures, including intense
pulsed light as well as radiofrequency procedures, are also increasing in popularity (see Chapters 16,17,18,19).
pulsed light as well as radiofrequency procedures, are also increasing in popularity (see Chapters 16,17,18,19).
When considering cosmetic procedures in darker racial ethnic groups, clinicians should be cognizant of the special structural and physiologic differences in the skin of such individuals. These differences can significantly affect and influence surgical and cosmetic surgery outcomes. This chapter will review the structural and physiologic features of the skin of darker racial ethnic groups.
Subjective and Objective Assessment of Skin Color
In the late 19th century, Felix von Luschan developed a chromatic scale to classify skin color.7 The von Luschan scale consisted of 36 opaque glass tiles that could be compared with a subject’s skin, typically in a non–sun-exposed area. This scale was commonly used throughout the early part of the 20th century to classify skin types. Because of its subjective nature, it was considered highly problematic and was abandoned in the mid-20th century. However, von Luschan’s global depiction of regions largely populated by darker racial ethnic groups remains relatively accurate today (Fig. 2-1).
The assessment of skin color and the ability to monitor color changes over time or during treatment of skin conditions is no doubt an important tool in dermatology and cosmetic surgery. The perception of skin color, however, is highly subjective, being influenced by many factors. These include pigmentation, desquamation, cutaneous blood flow, physical exertion, anatomic site, and variation in ambient lighting.8
The Fitzpatrick skin type classification was developed in 1975 by dermatologist Dr. Thomas Fitzpatrick as a sun-reactive skin typing system to classify persons with white skin to select appropriate doses of ultraviolet-A (UVA) for phototherapy patients.9 The classification was subsequently modified to measure responses in various skin types to sunlight and ultraviolet radiation. It correlates the color of skin with its ability to tan or burn with ultraviolet light exposure. It is based on six categories, which include:
Type I (very white or freckled): Always burn
Type II (white): Usually burn
Type III (white to olive): Sometimes burn
Type IV (brown): Rarely burn
Type V (dark brown): Very rarely burn
Type VI (black): Never burn
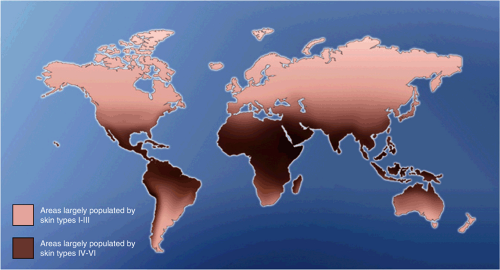 Figure 2-1 Global map depicting areas largely populated by individuals of darker racial ethnic heritage. Darker shaded areas of the global map represent areas largely populated by individuals of darker racial ethnic heritage. |
Darker racial ethnic groups are often classified as Fitzpatrick skin types IV through VI. Despite the fact that it was never designed for cosmetic purposes, the Fitzpatrick classification is often used as a criterion to determine the safety of a variety of cosmetic procedures in individuals with white, olive, brown, or black skin. As the American and global populations become increasingly diverse, the Fitzpatrick classification
has come under increasing scrutiny in its lack of ability to predict minimal erythema dosing (MED), minimum melanogenic dosing (MMD) to tanning, or even constitutive skin color. Multiple investigators are examining new scales to assess ultraviolet responses as well as scales that more accurately predict cosmetic surgery outcomes.10
has come under increasing scrutiny in its lack of ability to predict minimal erythema dosing (MED), minimum melanogenic dosing (MMD) to tanning, or even constitutive skin color. Multiple investigators are examining new scales to assess ultraviolet responses as well as scales that more accurately predict cosmetic surgery outcomes.10
New objective technologies have evolved that facilitate objective and reproducible quantitative measures of skin color and erythema. A variety of color-measuring instruments have evolved based on two different principles of color physics. These include reflectance spectrophotometry and tristimulus colorimetry.11 Spectrophotometer instruments use broad bands or selected wavelengths of light in the visible range and measure absorbance and reflectance. Tristimulus analysis of blue, red, and green light measures light reflection from skin structures. Convenient instruments using these principles include the Minolta Chromameter, the DermaSpectrometer, the Photovolt ColorWalk Colorimeter, the Mexameter, the DermaSpectrophotometer, and the Erythema Meter.
Grimes et al.12 measured the ranges of skin color and erythema by reflectance spectrophotometry in a multiracial population of 160 subjects including African Americans, Caucasians, Hispanics, Asians, and East Indians. Measurements were taken during the months of November through January, when summer tans had likely faded. There was a statistically significant correlation between reflectance spectrophotometry measurements using the Meximeter MX 16 (Courage Khazaka, Electronics, GMbH) and race and Fitzpatrick’s skin types (Fig. 2-2A, B). As the intensity of cutaneous pigmentation increased, measurements for melanin and erythema increased. There was no statistically significant correlation with age or sex. Additional studies are indeed warranted to further validate the reliability of bioinstrumentation as a tool for skin typing.
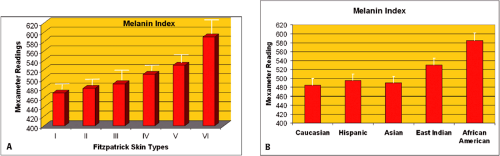 Figure 2-2 A: Reflectance spectrophotometry using the Mexameter MX16: correlation of melanin index with Fitzpatrick’s skin types. There was a statistically significant correlation (p = 0.01) between intensity of pigmentation (melanin index readings) and Fitzpatrick’s skin types. B: Reflectance spectrophotometery utilizing the Mexameter MX16: correlation of melanin index with race/ethnicity. There was a statistically significant correlation (p<0.05) between intensity of pigmentation (melanin index readings) and race. |
Melanocytes, Melanin, and Pigmentation
The key feature defining races is the color of an individual’s skin. Although skin color is influenced by melanin, hemoglobin in blood vessels, and dietary carotenoids, the predominant chromophore is melanin produced by melanocytes. The biologic differences observed in melanocytes and epidermal melanin have been well defined in black skin and white skin. Melanocytes are dendritic cells located in the basal layer of the epidermis (Fig. 2-3A,B). There are approximately 36 keratinocytes interfacing with 1 melanocyte, forming what is called an epidermal-melanin unit.13 The distribution of these cells varies in different regions of the body (Fig. 2-4). Melanocytes are more numerous on the head and neck, scrotum, foreskin, and dorsal feet.
The content of melanin within keratinocytes determines skin color, with deeply pigmented skin having the highest content of epidermal melanin (Fig. 2-5). Melanin is a dense, relatively insoluble polymer of high molecular weight. It exists in two forms: eumelanin and pheomelanin. Eumelanin is a highly cross-linked dark brown to black pigment predominantly responsible for skin pigmentation. Pheomelanin is a yellow-red alkali soluble pigment derived from tyrosine, in which dopaquinone combines with glutathione or cysteine to form cysteinyl-dopa. Pheomelanin is predominantly found in auburn or red-haired fair skinned individuals.
Melanin is synthesized on melanosomes via the Raper-Mason pathway (Fig. 2-6).14 The rate-limiting
enzyme for this process is tyrosine. Although the precise mechanism of transfer of melanosomes to keratinocytes is unknown, suggested mechanisms include (a) fusion of melanocyte and keratinocyte plasma membranes, (b) melanosome secretion into the intercellular space followed by keratinocyte endocytosis, and (c) phagocytosis of melanocyte dendritic tips by keratinocytes.15,16
enzyme for this process is tyrosine. Although the precise mechanism of transfer of melanosomes to keratinocytes is unknown, suggested mechanisms include (a) fusion of melanocyte and keratinocyte plasma membranes, (b) melanosome secretion into the intercellular space followed by keratinocyte endocytosis, and (c) phagocytosis of melanocyte dendritic tips by keratinocytes.15,16
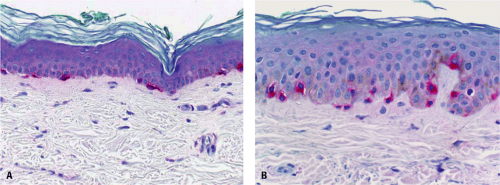 Figure 2-3 Immunohistochemical staining for melanocytes using an alkaline phosphatase detection kit and a 1:5 dilution of MEL-5 antibody after predigestion for 4 minutes with protease in (A) white skin and (B) black skin. |
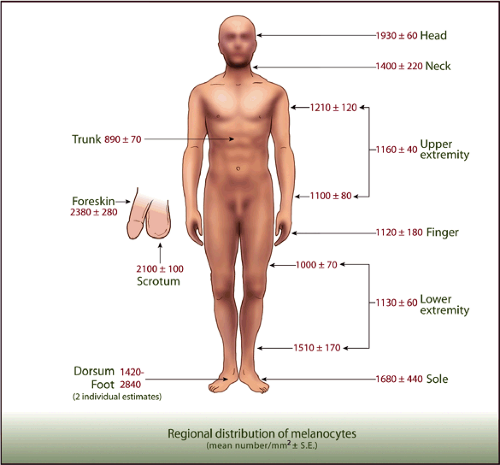 Figure 2-4 Anatomic distribution of melanocytes. (Modified from Fitzpatrick TB, Szabo G, Wick MM. Biochemistry and physiology of melanin pigment. In: Goldsmith LA, ed. Biochemistry and Physiology of the Skin. New York: Oxford Univ Press; 1983:112 . |
Melanosomes can occur as large, single membrane–bound mature melanosomes or as aggregates of smaller melanosomes. Although there are no quantitative differences
in melanocytes amongst various racial/ethnic groups, the skin of blacks has an increased content of epidermal melanin and large singly dispersed melanosomes within melanocytes and keratinocytes.17,18 Melanosomes have been identified in the entire epidermis, including the stratum granulosum, stratum lucidum, and stratum corneum. Pigmented skin in particular black skin has more stage IV melanosomes. In contrast, in very pale white skin, few melanosomes are seen in the basal keratinocytes and malpighian layer.19 However, darker-skinned Caucasians, upon skin exposure to sun, have
larger nonaggregated melanosomes. Lighter-complexioned blacks have a combination of large nonaggregated and smaller aggregated melanosome.19 In Asians, non–sun-exposed areas of skin have aggregated melanosomes, whereas sun-exposed areas have predominantly nonaggregated melanosomes.20 Such observations support the concept of significant intraracial and interracial variations in pigmentation.
in melanocytes amongst various racial/ethnic groups, the skin of blacks has an increased content of epidermal melanin and large singly dispersed melanosomes within melanocytes and keratinocytes.17,18 Melanosomes have been identified in the entire epidermis, including the stratum granulosum, stratum lucidum, and stratum corneum. Pigmented skin in particular black skin has more stage IV melanosomes. In contrast, in very pale white skin, few melanosomes are seen in the basal keratinocytes and malpighian layer.19 However, darker-skinned Caucasians, upon skin exposure to sun, have
larger nonaggregated melanosomes. Lighter-complexioned blacks have a combination of large nonaggregated and smaller aggregated melanosome.19 In Asians, non–sun-exposed areas of skin have aggregated melanosomes, whereas sun-exposed areas have predominantly nonaggregated melanosomes.20 Such observations support the concept of significant intraracial and interracial variations in pigmentation.
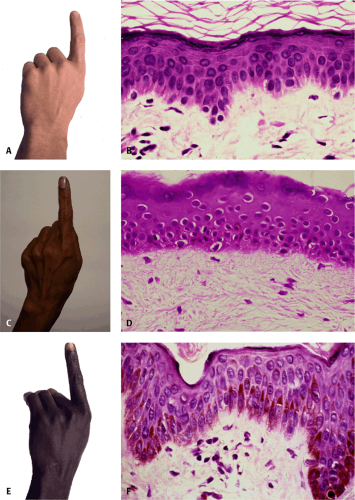 Figure 2-5 Photos and biopsies (40X magnification) taken from the hand of (A) and (B) Caucasians, (C) and (D) East Indians, and (E) and (F) African Americans. Note the progressive increase in melanin as skin pigmentation darkens. Courtesy of Jag Bhawan, MD. |
Recent work suggests that the expression and activation of protease-activated receptor-2 (PAR-2) correlates with skin color and may influence ethnic skin color phenotypes. PAR-2 receptors are expressed on keratinocytes. They have been shown to play a role in controlling melanosome ingestion and phagocytosis by keratinocytes.21,22 In addition, PAR-2 may play a regulatory role in skin pigmentation.23,24 Babiarz-Magee et al.21 examined the expression of PAR-2 and its activator trypsin in human skin from individuals with different shades of pigmentation. These findings suggest PAR-2 and trypsin were expressed in higher levels in darker compared with lighter skin. In addition, darker skin showed an increase in PAR-2 specific protease cleavage ability. These findings suggested that PAR-2 expression and activity may play an important role in ethnic skin color phenotypes.
A study comparing the transmission of ultraviolet radiation (UVA and UVB) through skin samples of blacks and whites using both biologic and spectroscopic techniques found that, on average, five times as much ultraviolet light reached the upper dermis of white skin as compared with black skin.25 Differences in transmission between the stratum corneum of blacks and of whites were far less striking. The main site of UV filtration in whites was the stratum corneum, whereas in blacks, it was the malpighian layers of the epidermis. The main UV protective factor for black epidermis was 13.14 compared with 3.4 for white skin.25
Rijken et al.26 investigated the responses of black and white skin to solar-simulating radiation. In subjects with skin types I to III, 12,000 to 18,000 mJ per cm2




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
